

Clinical Characteristics and Hypokalemia Risk Prediction in Patients With Hyperosmolar Hyperglycemic State and Diabetic Ketoacidosis (HHS-DKA): A Single-Center, Retrospective Observational Study
- PMID: 40546498
- PMCID: PMC12182720
- DOI: 10.7759/cureus.84672
Clinical Characteristics and Hypokalemia Risk Prediction in Patients With Hyperosmolar Hyperglycemic State and Diabetic Ketoacidosis (HHS-DKA): A Single-Center, Retrospective Observational Study
Abstract
Background: People with combined diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) often present with more severe metabolic derangements than those with DKA or HHS alone. This study aimed to clarify the clinical characteristics of HHS-DKA and explore predictive models for complications, including hypokalemia.
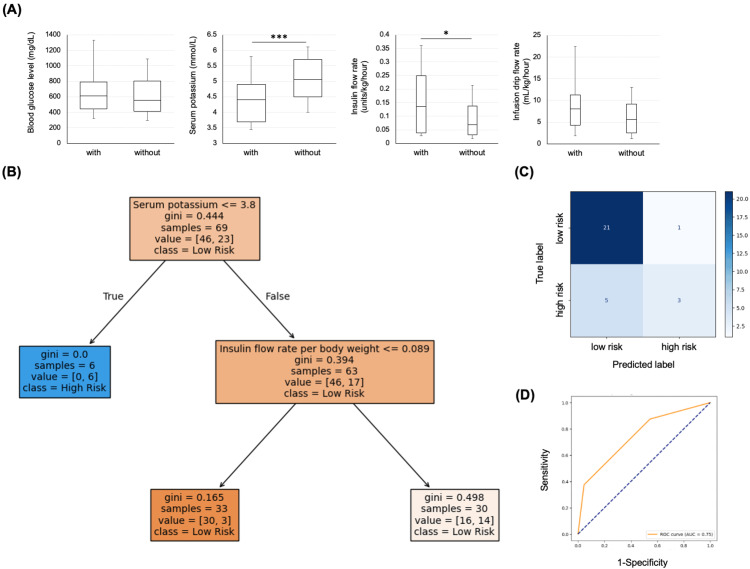
Methods: We retrospectively analyzed data from 99 patients admitted with hyperglycemic emergencies between April 1, 2010, and October 31, 2024, and classified them into DKA, HHS, and HHS-DKA groups. A decision tree model was also developed to predict the risk of post-continuous insulin infusion (CII) hypokalemia. The decision tree model was created using machine learning with the Python language (Python Software Foundation, Wilmington, Delaware).
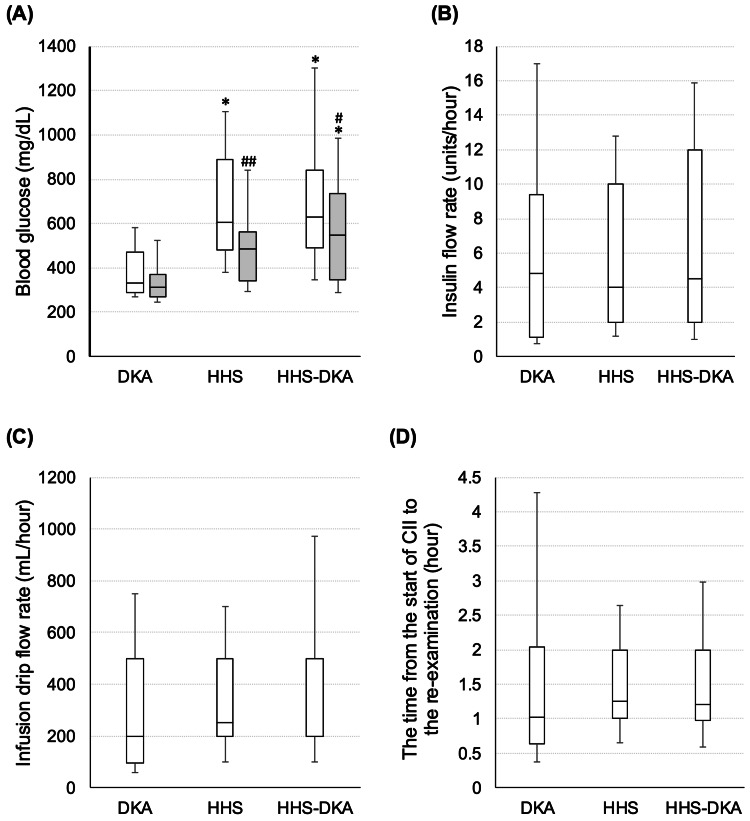
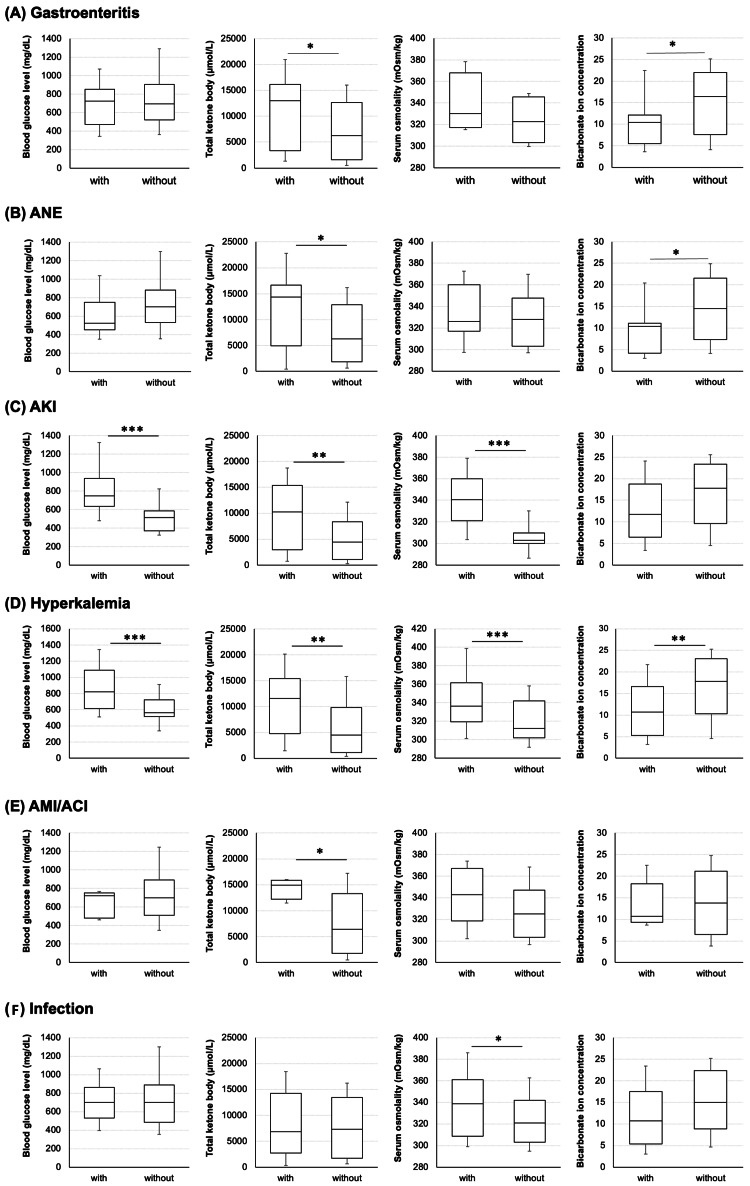
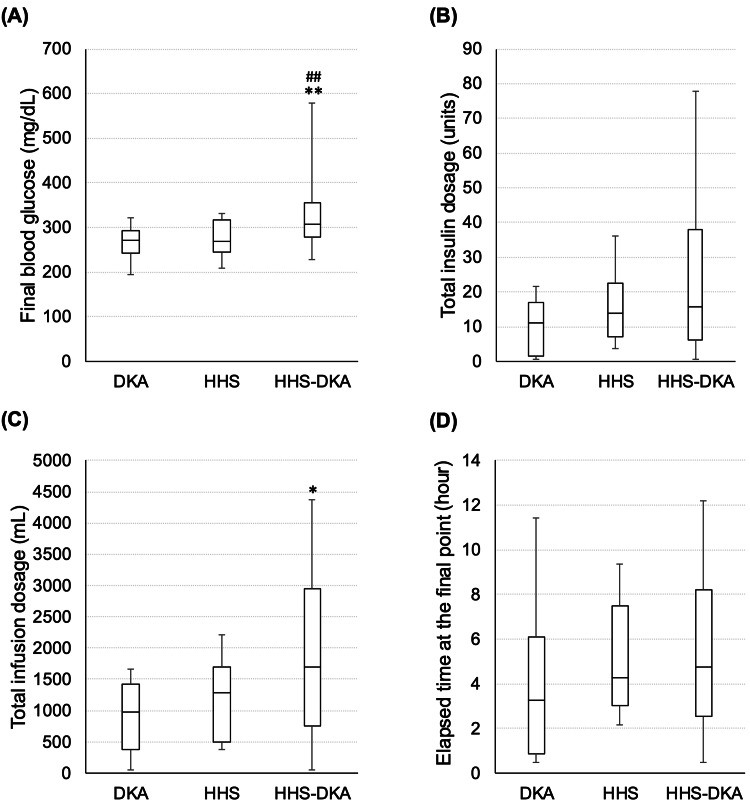
Results: HHS-DKA patients had significantly higher rates of acute kidney injury (84%) and hyperkalemia (58%) compared to those with DKA or HHS alone. A decision tree model predicted post-CII hypokalemia with 80% accuracy, identifying key predictors such as initial blood glucose and insulin flow rates.
Conclusion: HHS-DKA represents a distinct and severe clinical entity with unique characteristics and complications. Predictive models developed in this study will likely assist in risk stratification and improve patient management during hyperglycemic crises in emergency settings. However, as this was a single-center retrospective study without external validation, further studies are warranted to confirm these findings.
Keywords: continuous insulin infusion therapy; diabetes mellitus; diabetic ketoacidosis (dka); hyperosmolar hyperglycemic state (hhs); retrospective observational study.
Copyright © 2025, Iwamoto et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Review Board of Kawasaki Medical School issued approval 6229-00. The protocol for the research project has been approved by the Institutional Review Board of Kawasaki Medical School (No.: 6229-00). Ethical consideration or informed consent of the patient: Consent was obtained for participants in this study via opt-out on the Kawasaki Medical School website. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: Shuhei Nakanishi declare(s) personal fees from Novo Nordisk Pharma, Kowa and Daiichi Sankyo. S.N. has received honoraria for lectures from Novo Nordisk Pharma, Kowa, and Daiichi Sankyo. Kohei Kaku declare(s) a grant, personal fees and non-financial support from Novo Nordisk Pharma, Sanwa Kagaku, Taisho Pharma, Sumitomo Pharma, Astellas, Boehringer Ingelheim. K.K. has been an advisor to, received honoraria for lectures from, and received scholarship grants from Novo Nordisk Pharma, Sanwa Kagaku, Taisho Pharma, Sumitomo Pharma, Astellas, and Boehringer Ingelheim. Tomohiko Kimura declare(s) personal fees from Sumitomo Pharma and Novo Nordisk Pharma. T.K. has received honoraria for lectures from Sumitomo Pharma and Novo Nordisk Pharma. Hideaki Kaneto declare(s) a grant and personal fees from Novo Nordisk Pharma, Sanofi, Eli Lilly, Boehringer Ingelheim, Sumitomo Pharma, Daiichi Sankyo, Mitsubishi Tanabe Pharma, Manpei Suzuki Diabetes Foundation, Japan Arteriosclerosis Prevention Fund, Japan Association for Diabetes Education and Care. H.K. has received honoraria for lectures, received scholarship grants from Novo Nordisk Pharma, Sanofi, Eli Lilly, Boehringer Ingelheim, Sumitomo Pharma, Daiichi Sankyo, Mitsubishi Tanabe Pharma, Manpei Suzuki Diabetes Foundation, Japan Arteriosclerosis Prevention Fund, and Japan Association for Diabetes Education and Care. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Association between bipolar disorder and diabetic ketoacidosis/hyperosmolar hyperglycemic state.Sci Rep. 2025 Jul 2;15(1):22701. doi: 10.1038/s41598-025-08087-y. Sci Rep. 2025. PMID: 40596274 Free PMC article.
-
The effect of renal function on the clinical outcomes and management of patients hospitalized with hyperglycemic crises.Front Endocrinol (Lausanne). 2025 Jan 9;15:1445040. doi: 10.3389/fendo.2024.1445040. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39850482 Free PMC article.
-
Combined diabetic ketoacidosis and hyperosmolar hyperglycemic state in type 1 diabetes mellitus induced by immune checkpoint inhibitors: Underrecognized and underreported emergency in ICIs-DM.Front Endocrinol (Lausanne). 2023 Jan 4;13:1084441. doi: 10.3389/fendo.2022.1084441. eCollection 2022. Front Endocrinol (Lausanne). 2023. PMID: 36686495 Free PMC article.
-
Diabetic ketoacidosis and hyperglycaemic hyperosmolar syndrome in patients with cancer: A multicentre study.Clin Med (Lond). 2025 Jan;25(1):100262. doi: 10.1016/j.clinme.2024.100262. Epub 2024 Nov 9. Clin Med (Lond). 2025. PMID: 39522614 Free PMC article.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
References
-
- Characteristics and outcomes of the hyperglycemic hyperosmolar non-ketotic syndrome in a cohort of 51 consecutive cases at a single center. Fadini GP, de Kreutzenberg SV, Rigato M, Brocco S, Marchesan M, Tiengo A, Avogaro A. Diabetes Res Clin Pract. 2011;94:172–179. - PubMed
-
- Hyperosmolarity and acidosis in diabetes mellitus: a three-year experience in Rhode Island. Wachtel TJ, Tetu-Mouradjian LM, Goldman DL, Ellis SE, O'Sullivan PS. J Gen Intern Med. 1991;6:495–502. - PubMed
-
- Acute metabolic emergencies in diabetes: DKA, HHS and EDKA. Muneer M, Akbar I. Adv Exp Med Biol. 2021;1307:85–114. - PubMed
-
- Diabetic ketoacidosis. Dhatariya KK, Glaser NS, Codner E, Umpierrez GE. Nat Rev Dis Primers. 2020;6:40. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous