

Rapidly Evolving Cervical Dermatofibrosarcoma Protuberans With Deep Muscle Infiltration: A Rare and Aggressive Presentation
- PMID: 40546645
- PMCID: PMC12181793
- DOI: 10.7759/cureus.84596
Rapidly Evolving Cervical Dermatofibrosarcoma Protuberans With Deep Muscle Infiltration: A Rare and Aggressive Presentation
Abstract
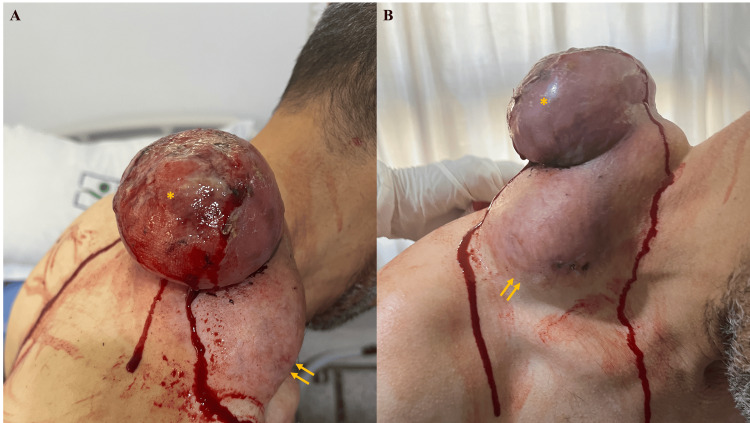
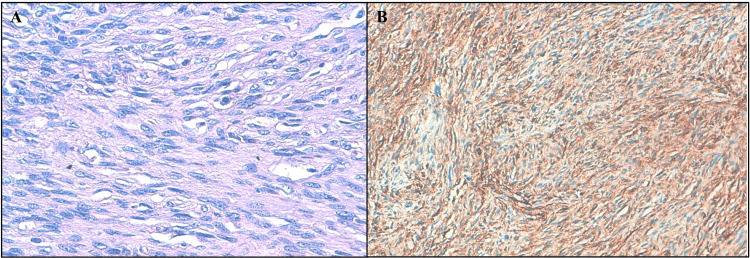
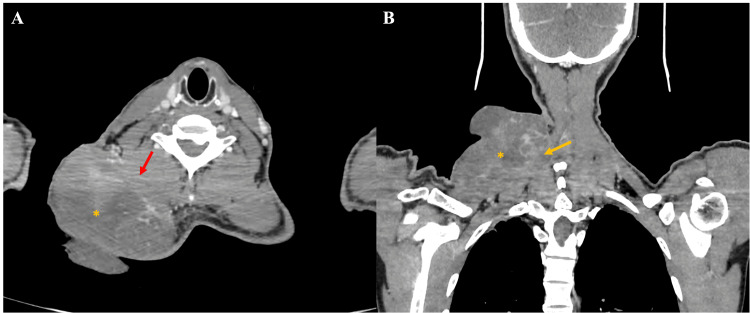
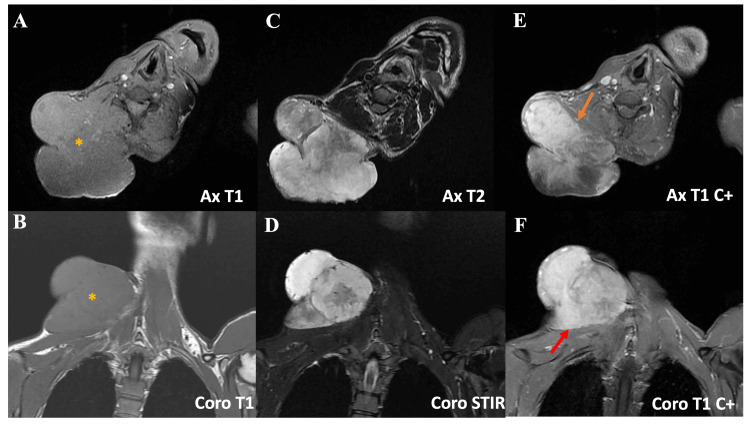
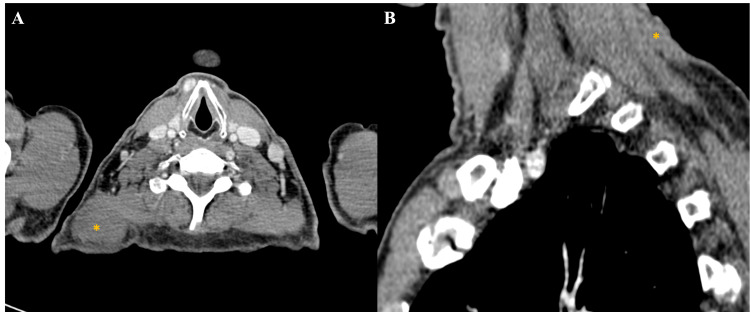
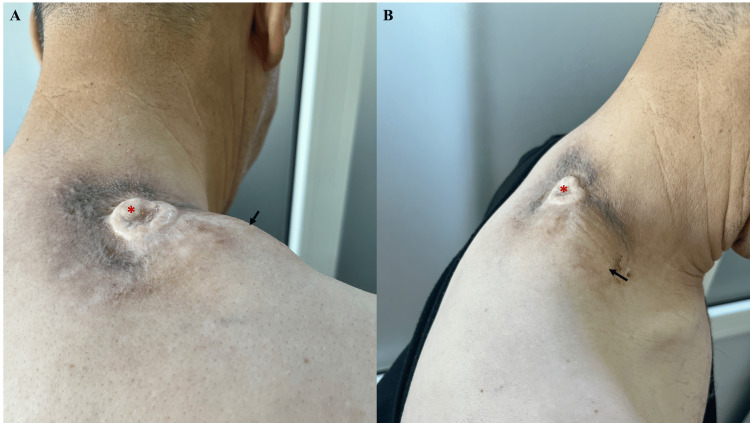
Dermatofibrosarcoma protuberans (DFSP) is a rare, low-grade sarcoma that typically presents as a slow-growing cutaneous nodule or plaque. We report a highly unusual case of DFSP involving the neck, which demonstrated rapid enlargement, necrosis, and deep muscle infiltration. A 45-year-old man presented with a large, bleeding cervical tumor that had evolved over two years. Imaging revealed extensive involvement of the neck and shoulder musculature without distant metastasis. Histopathologic evaluation confirmed the diagnosis of DFSP. Given the tumor's inoperability, treatment with imatinib was initiated, resulting in marked tumor regression. This case highlights an atypical presentation of DFSP in terms of both location and clinical behavior. It underscores the importance of repeated histologic assessment in the face of rapid progression, the role of imaging in surgical planning, and the value of targeted therapy when surgical options are limited.
Keywords: darier–ferrand dermatofibrosarcoma; dermatofibrosarcoma protuberans; imatinib mesylate; imatinib therapy; oncodermatology.
Copyright © 2025, Bouraqqadi et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Uncommon presentation of dermatofibrosarcoma protuberans: extensive growth in a rare location with subclinical cutaneous manifestation-a case report.Case Reports Plast Surg Hand Surg. 2025 Jul 26;12(1):2535699. doi: 10.1080/23320885.2025.2535699. eCollection 2025. Case Reports Plast Surg Hand Surg. 2025. PMID: 40727034 Free PMC article.
-
Impact of Dermatology Access on Dermatofibrosarcoma Protuberans Outcomes: A Retrospective Study in a Larger Cohort.S D Med. 2025 May;78(suppl 5):s30. S D Med. 2025. PMID: 40550169
-
Successful treatment of metastatic dermatofibrosarcoma protuberans of the breast to the lungs with imatinib mesylate: a case report.Ecancermedicalscience. 2025 May 27;19:1912. doi: 10.3332/ecancer.2025.1912. eCollection 2025. Ecancermedicalscience. 2025. PMID: 40556795 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Interventions targeted at women to encourage the uptake of cervical screening.Cochrane Database Syst Rev. 2021 Sep 6;9(9):CD002834. doi: 10.1002/14651858.CD002834.pub3. Cochrane Database Syst Rev. 2021. PMID: 34694000 Free PMC article.
References
-
- Low recurrence rate after surgery for dermatofibrosarcoma protuberans: a multidisciplinary approach from a single institution. DuBay D, Cimmino V, Lowe L, Johnson TM, Sondak VK. Cancer. 2004;100:1008–1016. - PubMed
-
- Dermatofibrosarcoma protuberans: what is this? Vitiello GA, Lee AY, Berman RS. Surg Clin North Am. 2022;102:657–665. - PubMed
-
- The epidemiology of dermatofibrosarcoma protuberans incidence, metastasis, and death among various population groups: a surveillance, epidemiology, and end results database analysis. Maghfour J, Genelin X, Olson J, Wang A, Schultz L, Blalock TW. J Am Acad Dermatol. 2024;91:826–833. - PubMed
Publication types
LinkOut - more resources
Full Text Sources