

Long-Segment Ventral Spinal Epidural Abscesses Caused by Mycobacterium Tuberculosis: A Report of 2 Cases and Review
- PMID: 40547101
- PMCID: PMC12178294
- DOI: 10.2106/JBJS.OA.24.00249
Long-Segment Ventral Spinal Epidural Abscesses Caused by Mycobacterium Tuberculosis: A Report of 2 Cases and Review
Abstract
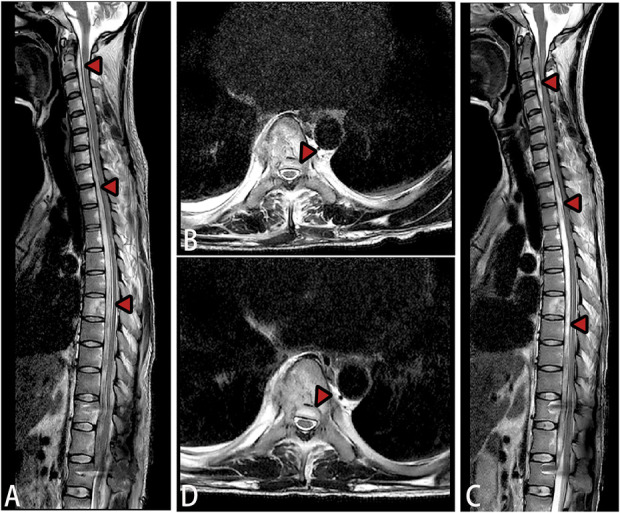
» Abscesses caused by spinal tuberculosis typically occur in the anterior and lateral regions of the vertebral bodies, often extending to the paraspinal muscles as cold abscesses. Although intraspinal abscesses due to spinal tuberculosis are very common, cases with longitudinally extensive abscesses in the ventral epidural space of the spinal cord are not well-documented. The disease is characterized by insidious onset, rapid progression, and a high risk of irreversible neurological damage, highlighting the necessity for early diagnosis and prompt treatment. » This review presents 2 rare cases of long-segment tuberculous spinal epidural abscesses, with both patients achieving significant symptom improvement after precise surgical intervention and standardized antituberculosis therapy. A long-segment tuberculous spinal epidural abscess (SEA) is an extremely rare complication that may cause severe neurological impairment, and magnetic resonance imaging revealed extensive spinal epidural abscesses. Clinical manifestations, such as neck stiffness, can easily be mistaken for tuberculous encephalopathy; therefore, contrast-enhanced MRI is recommended to differentiate a SEA from tuberculous encephalopathy. » Local decompression with catheter drainage can help preserve neurological function, establish a definitive etiological diagnosis, and guide subsequent treatment. Early, adequate, and comprehensive antituberculosis therapy is crucial for successful management.
Copyright © 2025 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
All patients consented to their data being used anonymously. The Clinical Ethics Committee of our hospital approved this retrospective study (2024-ER-076). The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A818).
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases