

Necrotic Thymoma Discovered Due to Subjective Symptoms: A Report of Three Cases
- PMID: 40547416
- PMCID: PMC12180143
- DOI: 10.70352/scrj.cr.25-0216
Necrotic Thymoma Discovered Due to Subjective Symptoms: A Report of Three Cases
Abstract
Introduction: Thymomas are solid tumors that usually grow slowly and rarely cause symptoms or spontaneously regression. We have observed three cases of thymoma in which the patient presented with fever and chest pain, and pathological examination showed relatively extensive necrosis. The tumors spontaneously shrank during the course of the diseases.
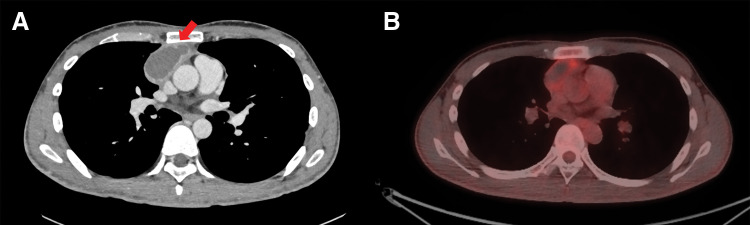
Case presentation: The patients, of a 30-year-old man, 46-year-old man, and 76-year-old man presented with fever and/or chest pain, and blood tests showed high levels of inflammation. Contrast-enhanced chest computed tomography (CT) showed masses with low-density area and contrast-enhanced margins. Two patients had repeat chest CT just prior to surgery, and the tumors had shrunk. In all cases, the masses were removed by a median sternotomy. The mediastinum tissue was hard due to inflammation, and in all cases the tumors were adherent to the lungs and in one case wedge resection of the left lung was required. Histopathological examination revealed extensive necrosis of the tumors, and based on residual viable tumor cells, the three tumors were diagnosed as follows respectively; type B2, type B2 with some type B3 components, and type AB thymoma. All tumors were classified as pT1aN0M0, Stage I, and Masaoka stage II.
Conclusions: Necrotic thymoma is associated with inflammation and spontaneous regression may be observed during the course of the disease. Since necrosis can be extensive, pathological examination should be performed throughout.
Keywords: mediastinal tumor; necrotic thymoma; spontaneous regression.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
References
-
- Takasaki C, Ishibashi H, Fujiwara N, et al. A case of thymoma with chest pain caused by bleeding necrosis. J Jpn Assoc Chest Surg 2012; 6: 45–8. (in Japanese)
-
- Moran CA, Suster S. Thymoma with prominent cystic and hemorrhagic changes and areas of necrosis and infarction: a clinicopathologic study of 25 cases. Am J Surg Pathol 2001; 25: 1086–90. - PubMed
-
- Kataoka Y, Okamoto K, Oshio M, et al. A case of thymoma with extensive necrosis. J Jpn Assoc Chest Surg 2015; 29: 627–31. (in Japanese)
-
- Yasukawa M, Kawaguchi T, Kawai N, et al. Spontaneous regression of thymoma: report of two cases. J Jpn Assoc Chest Surg 2017; 31: 36–41. (in Japanese)