

Epidural analgesia and rate of cesarean section, maternal and neonatal outcomes: Retrospective study
- PMID: 40547782
- PMCID: PMC12178526
- DOI: 10.4103/jfmpc.jfmpc_1508_24
Epidural analgesia and rate of cesarean section, maternal and neonatal outcomes: Retrospective study
Abstract
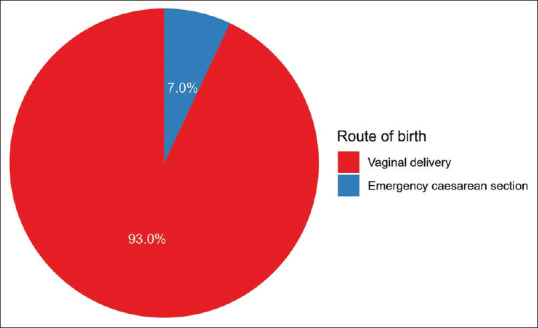
The neuraxial technique is standard medical care for labor pain relief. Epidural analgesia is linked to an increased likelihood of assisted vaginal birth but does not raise the overall cesarean section (CS) delivery risk. Few studies in the Middle East and Saudi Arabia have examined epidural analgesia's effect on emergency cesarean section rates among vaginal deliveries. This retrospective study at a tertiary care center in Saudi Arabia included 387 term pregnant women. Patients were divided into two groups: 240 received epidural analgesia, and 147 served as controls. Inclusion criteria included women aged 18-40 with specific fetal characteristics. Maternal and neonatal outcomes were analyzed using Chi-squared, Fisher's exact, and Wilcoxon tests. Women who received epidural analgesia were younger, with lower gravidity and parity, and had a higher rate of emergency cesarean sections. No significant differences were found in instrumental delivery rates, severe tears, or postpartum hemorrhage between groups. Neonatal outcomes, including Apgar scores, birth weight, and neonatal intensive care unit (NICU) admissions, were similar. Logistic regression indicated a higher likelihood of emergency CS with epidural analgesia, but this was insignificant in multivariable analysis. Gravidity and parity were inversely associated with emergency CS and instrumental deliveries. While epidural analgesia was linked to higher C-sections, further analysis showed no significant effect. Maternal and neonatal outcomes were similar between groups. These findings support the safe use of epidural analgesia for labor pain management in Saudi Arabia, offering reassurance to both patients and healthcare providers.
Keywords: Cesarean sections; NICU; epidural analgesia; instrumental deliveries; vaginal birth.
Copyright: © 2025 Journal of Family Medicine and Primary Care.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Epidural versus non-epidural or no analgesia for pain management in labour.Cochrane Database Syst Rev. 2018 May 21;5(5):CD000331. doi: 10.1002/14651858.CD000331.pub4. Cochrane Database Syst Rev. 2018. PMID: 29781504 Free PMC article.
-
Acupuncture or acupressure for induction of labour.Cochrane Database Syst Rev. 2017 Oct 17;10(10):CD002962. doi: 10.1002/14651858.CD002962.pub4. Cochrane Database Syst Rev. 2017. PMID: 29036756 Free PMC article.
-
Effects of Early and Late Labor Epidural Analgesia on Multiparous Women: A Retrospective Monocentric Study.Cureus. 2025 May 26;17(5):e84825. doi: 10.7759/cureus.84825. eCollection 2025 May. Cureus. 2025. PMID: 40568290 Free PMC article.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
-
Position in the second stage of labour for women with epidural anaesthesia.Cochrane Database Syst Rev. 2017 Feb 24;2(2):CD008070. doi: 10.1002/14651858.CD008070.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2018 Nov 09;11:CD008070. doi: 10.1002/14651858.CD008070.pub4. PMID: 28231607 Free PMC article. Updated.
References
-
- Gizzo S, Noventa M, Fagherazzi S, Lamparelli L, Ancona E, Di Gangi S, et al. Update on best available options in obstetrics anaesthesia:Perinatal outcomes, side effects and maternal satisfaction. Fifteen years systematic literature review. Arch Gynecol Obstet. 2014;290:21–34. - PubMed
-
- Bucklin BA, Hawkins JL, Anderson JR, Ullrich FA. Obstetric anesthesia workforce survey:Twenty-year update. J Am Soc Anesthesiol. 2005;103:645–53. - PubMed
-
- Morishima HO. Labor analgesia in the US and Japan. Masui Jpn J Anesthesiol. 2007;56:1040–3. - PubMed
LinkOut - more resources
Full Text Sources