

Modeling the impact of hospitalization-induced behavioral changes on the spread of COVID-19 in New York City
- PMID: 40547859
- PMCID: PMC12181002
- DOI: 10.1016/j.idm.2025.05.001
Modeling the impact of hospitalization-induced behavioral changes on the spread of COVID-19 in New York City
Abstract
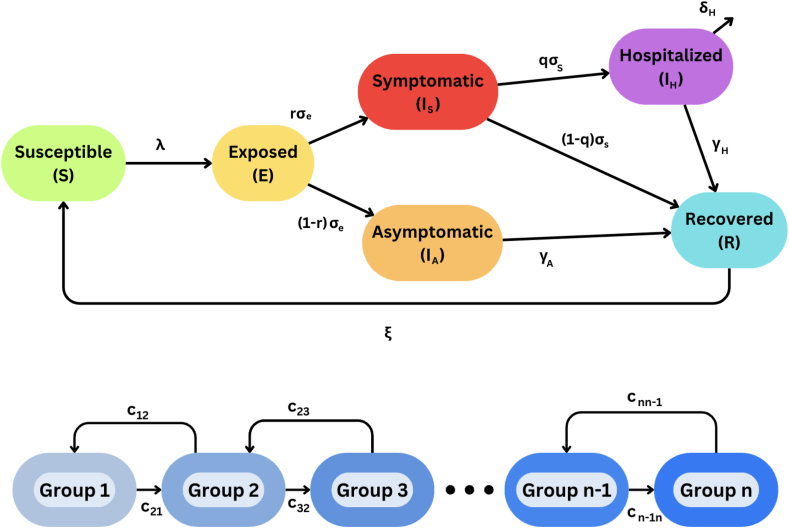
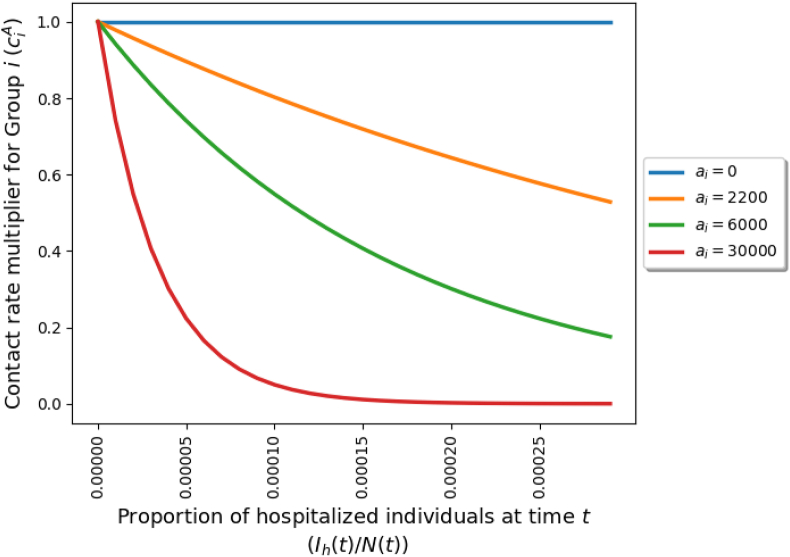
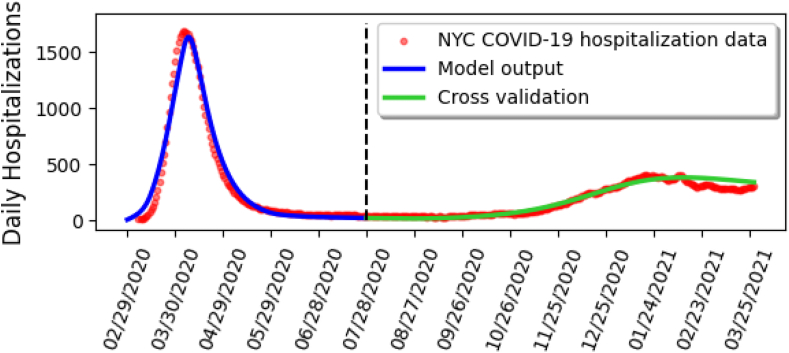
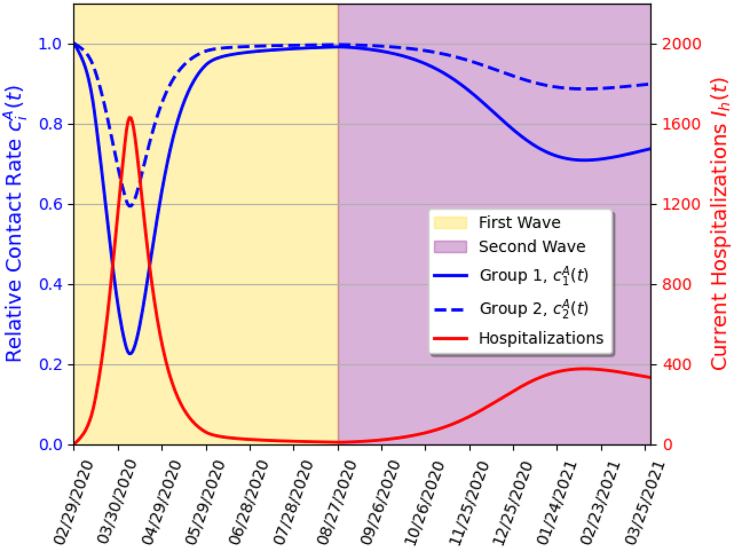
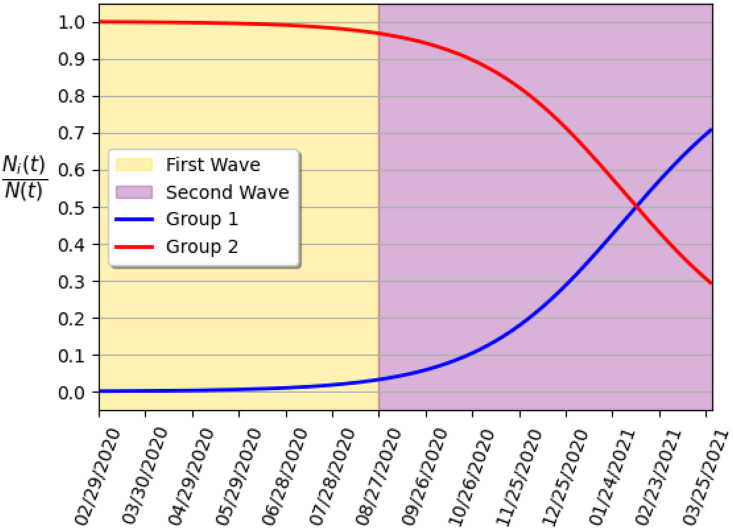
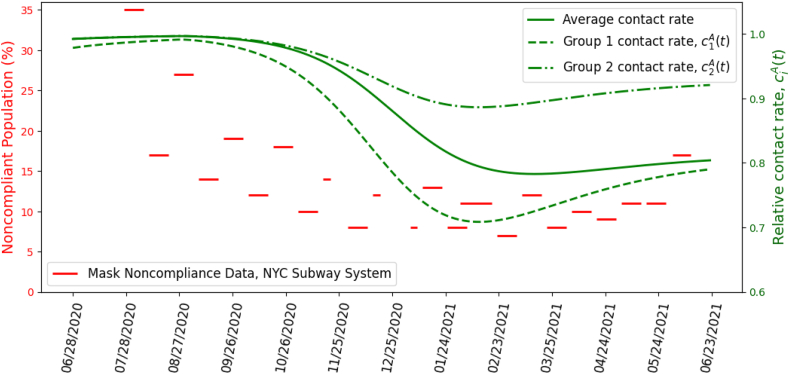
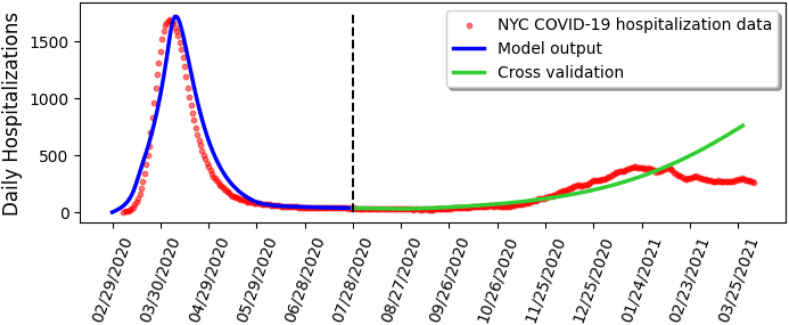
The COVID-19 pandemic, caused by SARS-CoV-2, highlighted heterogeneities in human behavior and attitudes of individuals with respect to adherence or lack thereof to public health-mandated intervention and mitigation measures. This study is based on using mathematical modeling approaches, backed by data analytics and computation, to theoretically assess the impact of human behavioral changes on the trajectory, burden, and control of the COVID-19 pandemic during the first two waves in New York City. A novel behavior-epidemiology model, which considers n heterogeneous behavioral groups based on level of risk tolerance and distinguishes behavioral changes by social and disease-related motivations (such as peer-influence and fear of disease-related hospitalizations), is developed. In addition to rigorously analyzing the basic qualitative features of this model, a special case is considered where the total population is stratified into two groups: risk-averse (Group 1) and risk-tolerant (Group 2). The 2-group model was calibrated and validated using daily hospitalization data for New York City during the first wave, and the calibrated model was used to predict the data for the second wave. The 2-group model predicts the daily hospitalizations during the second wave almost perfectly, compared to the version without behavioral considerations, which fails to accurately predict the second wave. This suggests that epidemic models of the COVID-19 pandemic that do not explicitly account for heterogeneities in human behavior may fail to accurately predict the trajectory and burden of the pandemic in a population. Numerical simulations of the calibrated 2-group behavior model showed that while the dynamics of the COVID-19 pandemic during the first wave was largely influenced by the behavior of the risk-tolerant (Group 2) individuals, the dynamics during the second wave was influenced by the behavior of individuals in both groups. It was also shown that disease-motivated behavioral changes (i.e., behavior changes due to the level of COVID-19 hospitalizations in the community) had greater influence in significantly reducing COVID-19 morbidity and mortality than behavior changes due to the level of peer or social influence or pressure. Finally, it is shown that the initial proportion of members in the community that are risk-averse (i.e., the proportion of individuals in Group 1 at the beginning of the pandemic) and the early and effective implementation of non-pharmaceutical interventions have major impacts in reducing the size and burden of the pandemic (particularly the total COVID-19 mortality in New York City during the second wave).
Keywords: Behavioral-epidemiology model; COVID-19; Equilibria; Influence dynamics.
© 2025 The Authors.
Conflict of interest statement
The author is an Editorial Board Member/Editor-in-Chief/Associate Editor/Guest Editor for Infectious Disease Modelling and was not involved in the editorial review or the decision to publish this article.
Figures
Similar articles
-
Measures implemented in the school setting to contain the COVID-19 pandemic.Cochrane Database Syst Rev. 2022 Jan 17;1(1):CD015029. doi: 10.1002/14651858.CD015029. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 May 2;5:CD015029. doi: 10.1002/14651858.CD015029.pub2. PMID: 35037252 Free PMC article. Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Surveillance of Barrett's oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.Health Technol Assess. 2006 Mar;10(8):1-142, iii-iv. doi: 10.3310/hta10080. Health Technol Assess. 2006. PMID: 16545207
References
-
- Akaike H. A new look at the statistical model identification. IEEE Transactions on Automatic Control. 1974;19(6)
-
- Amid ongoing COVID-19 pandemic Governor Cuomo announces New York City playgrounds will close. 2020. https://www.governor.ny.gov/news/video-audio-rush-transcript-amid-ongoin... Available at:
-
- Amid ongoing COVID-19 pandemic, Governor Cuomo announces NYS on pause functions extended for additional two weeks. 2020. https://www.governor.ny.gov/news/amid-ongoing-covid-19-pandemic-governor... Available at:
-
- Anderson R.M., May R.M. Oxford University Press; 1992. Infectious diseases of humans: Dynamics and control.
LinkOut - more resources
Full Text Sources
Miscellaneous
