

Optimal Tightrope Positioning for Adequate Syndesmotic Stabilization in Simulated Syndesmotic Injuries
- PMID: 40547897
- PMCID: PMC12179484
- DOI: 10.1177/24730114251342243
Optimal Tightrope Positioning for Adequate Syndesmotic Stabilization in Simulated Syndesmotic Injuries
Abstract
Background: Use of syndesmotic suture button fixation has gained in popularity for treating an injury to the tibiofibular syndesmosis. This biomechanical study used a cadaveric model to simulate in vivo loading conditions to assess the impact of the placement of a syndesmotic stabilization construct using a suture button device.
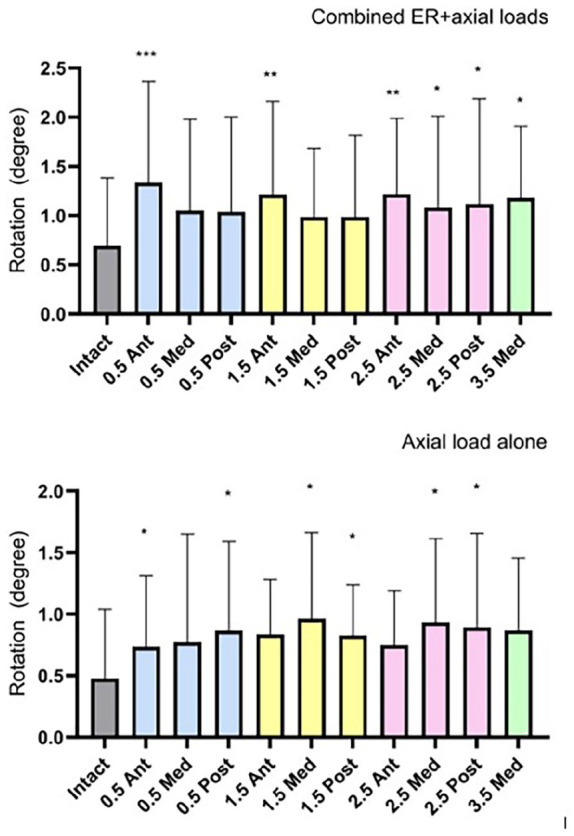
Methods: Biomechanical fixation stability with suture button device (TightRope; Arthrex, Naples, FL) placed at 4 distances from the tibiotalar joint line (0.5, 1.5, 2.5, and 3.5 cm) and 3 trajectories (anterior, medial, and posterior) were studied using cadaveric lower extremities with created syndesmotic injuries. Nondestructive testing was conducted on a biaxial servo-hydraulic load frame. The load application consisted of 2 portions: (1) axial compression simulating weightbearing and (2) external rotation of the ankle (up to 12 degrees and under 7.5 Nm) around the long axis of the tibia combined with weightbearing. Fibular motion and syndesmotic widening were tracked using motion analysis to quantify stability.
Results: Fixation placed at 0.5 or 1.5 cm from the joint line in medial or posterior trajectories resulted in the lowest increases in fibular rotation under loading. More proximal or anterior placements led to increased fibular motion and decreased rotational stability. Ankle width changes were minimal in most groups, although slightly increased widening occurred at proximal and anterior placements.
Conclusion: Placement of the syndesmotic suture button fixation 0.5-1.5 cm of the joint line in medial or posterior orientations provides the most rotationally stable fixation in a cadaveric model. These findings support flexibility in syndesmotic suture button fixation positioning when hardware constraints limit ideal placement.
Keywords: ankle fracture; biomechanical; suture button; syndesmosis.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alex T. Burton, MD, received a grant from Arthrex (IRR-01718) to supply the tightropes necessary for the study. Disclosure forms for all authors are available online.
Figures



References
LinkOut - more resources
Full Text Sources