

Evaluating inhaled corticosteroids' impact on osteoporosis and fracture risk in COPD patients: a real-world evidence-based systematic review and meta-analysis
- PMID: 40547916
- PMCID: PMC12178898
- DOI: 10.3389/fmed.2025.1503475
Evaluating inhaled corticosteroids' impact on osteoporosis and fracture risk in COPD patients: a real-world evidence-based systematic review and meta-analysis
Abstract
Background: The impact of current inhaled corticosteroid (ICS) therapies on fracture risk in patients with chronic obstructive pulmonary disease (COPD) remains uncertain.
Objective: This study conducts a systematic review and meta-analysis to assess the risk of fractures associated with ICS use over at least 4 years, synthesizing evidence from observational studies conducted in real-world settings among individuals with COPD.
Methods: We systematically searched PubMed, EMBASE, Scopus, and Web of Science from inception to April 21, 2025. Inclusion criteria encompassed studies conducted in COPD patients, evaluating interventions involving ICS-containing treatments compared to alternatives or no ICS use, using cohort or case-control designs, and reporting outcomes related to osteoporosis or fractures. Pooled odds ratios (OR) and hazard ratios (HR) were calculated using random-effects models. Subgroup analyses and meta-regression were performed to explore sources of heterogeneity.
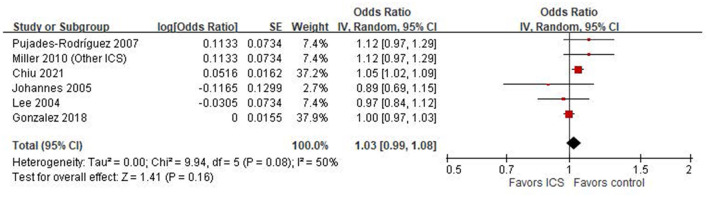
Results: Nine studies (six case-control, three cohort) were included. The pooled OR from case-control studies was 1.03 (95% CI: 0.99-1.08; I 2 = 50%), and the pooled HR from cohort studies was 0.95 (95% CI: 0.67-1.33; I 2 = 86%). Subgroup analyses indicated a potential increased risk in Asian and European populations but not in North America. Meta-regression revealed that higher oral corticosteroids exposure was significantly associated with increased risk (p = 0.005, R 2 = 100%).
Conclusions: Although ICS did not significantly impact osteoporosis or fracture risk, these are common comorbidities in COPD patients. Methodological differences, such as study design, outcome definitions, and oral corticosteroids use, may influence result interpretation and contribute to heterogeneity, limiting study comparability.
Keywords: chronic obstructive pulmonary disease; fracture; inhaled corticosteroids; meta-analysis; osteoporosis; systematic review.
Copyright © 2025 Huang, Hsu, Hsieh and Liao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Interventions to improve adherence to inhaled steroids for asthma.Cochrane Database Syst Rev. 2017 Apr 18;4(4):CD012226. doi: 10.1002/14651858.CD012226.pub2. Cochrane Database Syst Rev. 2017. PMID: 28417456 Free PMC article.
-
Inhaled corticosteroids for the treatment of COVID-19.Cochrane Database Syst Rev. 2022 Mar 9;3(3):CD015125. doi: 10.1002/14651858.CD015125. Cochrane Database Syst Rev. 2022. PMID: 35262185 Free PMC article.
-
Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 Aug 4;8(8):CD011682. doi: 10.1002/14651858.CD011682.pub2. Cochrane Database Syst Rev. 2017. PMID: 28777450 Free PMC article.
-
Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 May 23;5(5):CD011425. doi: 10.1002/14651858.CD011425.pub2. Cochrane Database Syst Rev. 2017. PMID: 28535331 Free PMC article.
-
Increased versus stable doses of inhaled corticosteroids for exacerbations of chronic asthma in adults and children.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD007524. doi: 10.1002/14651858.CD007524.pub5. Cochrane Database Syst Rev. 2022. PMID: 36161875 Free PMC article.
References
-
- Vestbo J, Anderson JA, Brook RD, Calverley PM, Celli BR, Crim C, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomised controlled trial. Lancet. (2016) 387:1817–26. 10.1016/S0140-6736(16)30069-1 - DOI - PubMed
-
- Calverley PMA, Anderson JA, Brook RD, Crim C, Gallot N, Kilbride S, et al. Fluticasone furoate, vilanterol, and lung function decline in patients with moderate chronic obstructive pulmonary disease and heightened cardiovascular risk. Am J Respir Crit Care Med. (2018) 197:47–55. 10.1164/rccm.201610-2086OC - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous