

Endoscopic-Assisted Fibula Reduction With Full Percutaneous Fixation of Ankle Fracture Dislocation
- PMID: 40547981
- PMCID: PMC12177375
- DOI: 10.1016/j.eats.2024.103398
Endoscopic-Assisted Fibula Reduction With Full Percutaneous Fixation of Ankle Fracture Dislocation
Abstract
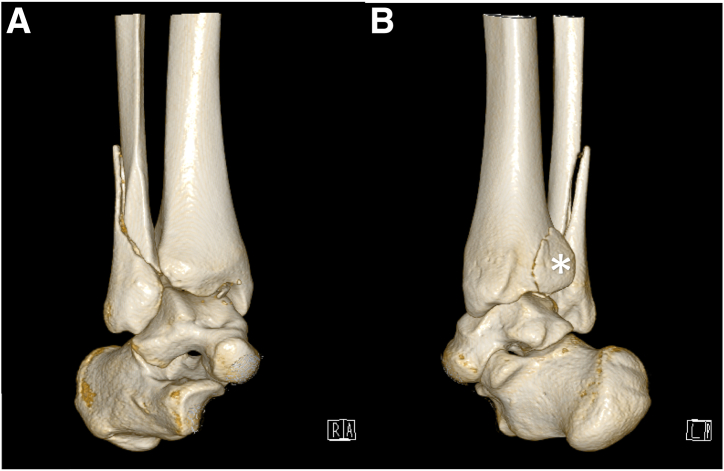
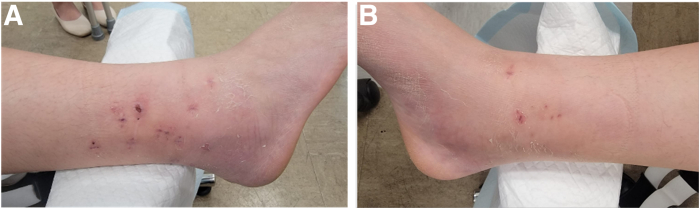
Ankle fracture is one of the most commonly encountered fractures. Open reduction and internal fixation is the gold standard of treatment. However, minimally invasive fixation of ankle fracture is gaining popularity among foot and ankle surgeons as the result of recent advances in ankle arthroscopic techniques. Despite this, there are limited reports on endoscopic assessment of fibula fracture. In this Technical Note, we describe an endoscopic-assisted fibula reduction with full percutaneous fixation of ankle fracture dislocation. Patients with noncomminuted fibula fracture or poor soft-tissue condition may be more indicated for minimally invasive ankle fracture fixation. This technique can provide better visualization of fibula fracture during percutaneous fixation and may result in less soft-tissue trauma.
© 2024 The Authors.
Conflict of interest statement
All authors (C.M.H., L.S.K.K.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures






Similar articles
-
Interventions for treating supracondylar elbow fractures in children.Cochrane Database Syst Rev. 2022 Jun 9;6(6):CD013609. doi: 10.1002/14651858.CD013609.pub2. Cochrane Database Syst Rev. 2022. PMID: 35678077 Free PMC article.
-
The role of intramedullary fixation in ankle fractures - A systematic review.Foot Ankle Surg. 2018 Feb;24(1):1-10. doi: 10.1016/j.fas.2016.04.004. Epub 2016 Apr 23. Foot Ankle Surg. 2018. PMID: 29413767
-
Can Locked Fibula Nail Replace Plate Fixation for Treatment of Acute Ankle Fracture? A Systematic Review and Meta-Analysis.J Foot Ankle Surg. 2023 Jan-Feb;62(1):178-185. doi: 10.1053/j.jfas.2022.10.003. Epub 2022 Oct 13. J Foot Ankle Surg. 2023. PMID: 36333182
-
Percutaneous Intramedullary Screw Fixation of Distal Fibula Fractures: A Case Series and Systematic Review.J Foot Ankle Surg. 2017 Sep-Oct;56(5):1081-1086. doi: 10.1053/j.jfas.2017.05.024. Epub 2017 Jun 21. J Foot Ankle Surg. 2017. PMID: 28647520
-
Clinical outcomes in the surgical management of ankle fractures: A systematic review and meta-analysis of fibular intramedullary nail fixation vs. open reduction and internal fixation in randomized controlled trials.Foot Ankle Surg. 2022 Oct;28(7):836-844. doi: 10.1016/j.fas.2022.03.009. Epub 2022 Mar 24. Foot Ankle Surg. 2022. PMID: 35339374
Cited by
-
Arthroscopic Fixation of Tibial Plafond Central Depression Pilon Fracture With Percutaneous Jail Screw Technique.Arthrosc Tech. 2025 Apr 15;14(6):103530. doi: 10.1016/j.eats.2025.103530. eCollection 2025 Jun. Arthrosc Tech. 2025. PMID: 40656725 Free PMC article.
References
-
- Scheer R.C., Newman J.M., Zhou J.J., et al. Ankle fracture epidemiology in the United States: Patient-related trends and mechanisms of injury. J Foot Ankle Surg. 2020;59:479–483. - PubMed
-
- Abdelgaid S.M., Moursy A.F., Elgebaly E.A.A., Aboelenien A.M. Minimally invasive treatment of ankle fractures in patients at high risk of soft tissue wound healing complications. J Foot Ankle Surg. 2018;57:557–571. - PubMed
-
- Yañez Arauz J.M. Minimally invasive treatment of AO B ankle fractures: Surgical technique and long-term outcomes. Foot Ankle Surg. 2021;27:742–749. - PubMed
LinkOut - more resources
Full Text Sources
