

Labral Scaffolding Technique Utilizing Dermal Allograft to Address Subcritical Glenoid Bone Loss in Glenoid Labrum Repair
- PMID: 40547993
- PMCID: PMC12177498
- DOI: 10.1016/j.eats.2025.103433
Labral Scaffolding Technique Utilizing Dermal Allograft to Address Subcritical Glenoid Bone Loss in Glenoid Labrum Repair
Abstract
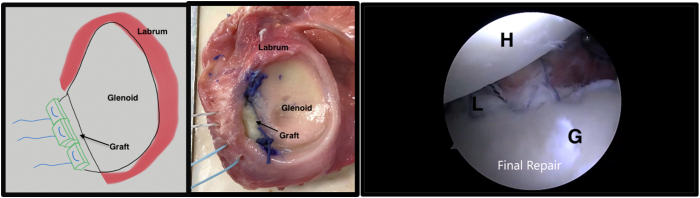
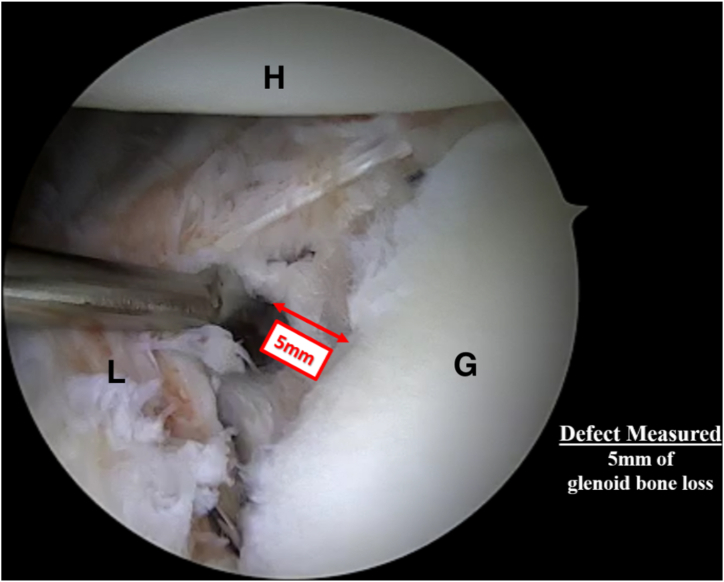
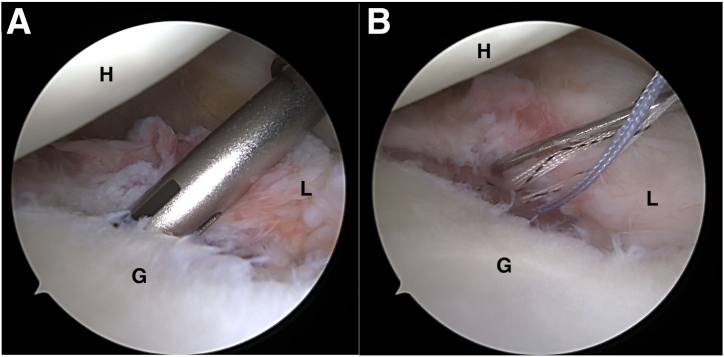
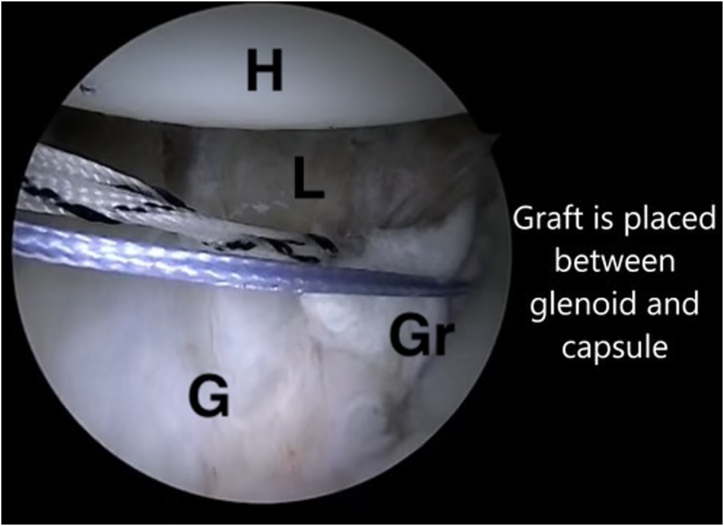
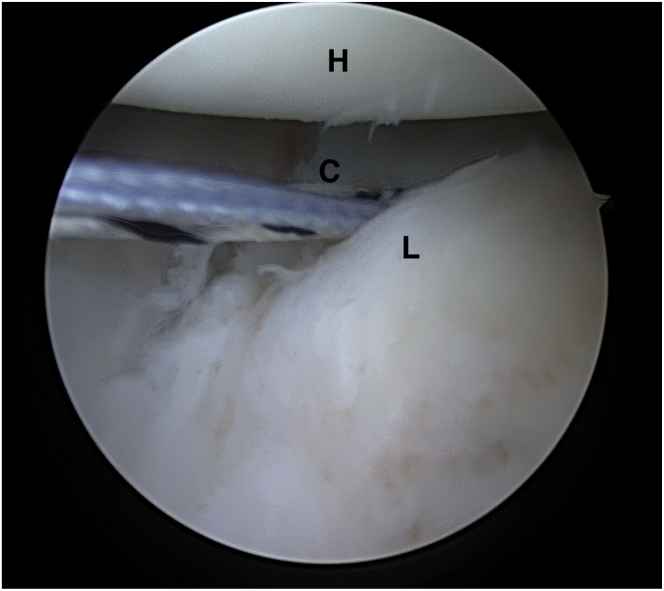
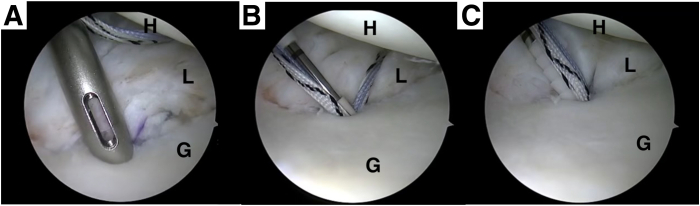
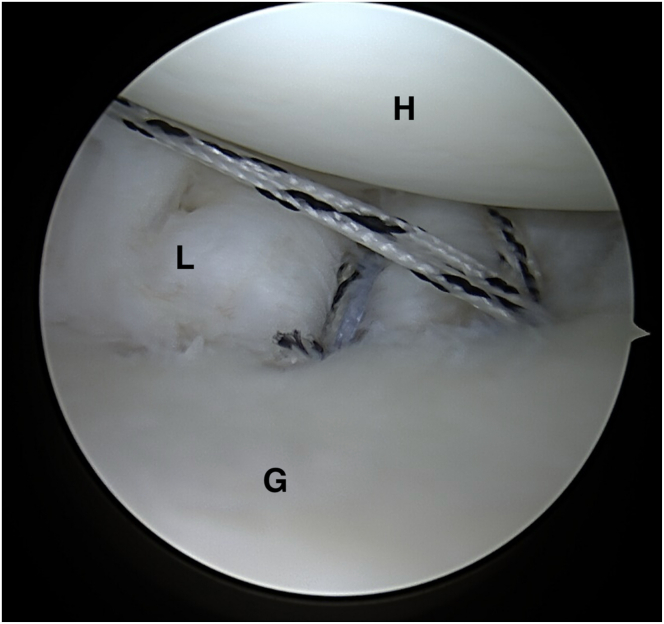
A treatment gap exists in the treatment of shoulder instability with subcritical bone loss. In this population, standard arthroscopic labral repairs have been associated with high failure rates. Bone block procedures are associated with low rates of recurrent instability but are associated with a high complication rate and subsequent long-term degenerative changes, making its use less than optimal in subcritical bone loss. We describe the arthroscopic "labral scaffold" technique using dermal allograft with labral reconstruction to address subcritical glenoid bone loss. This technique utilizes a dermal allograft to augment the bony deficit to better restore more native glenohumeral biomechanics with a double-row labral repair and subsequent labral reconstruction.
© 2025 The Authors.
Conflict of interest statement
All authors (S.Q., J.A., D.W., S.A.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures










References
-
- Min K.S., Horng J., Cruz C., Ahn H.J., Patzkowski J. Glenoid bone loss in recurrent shoulder instability after arthroscopic Bankart repair: A systematic review. J Bone Joint Surg Am. 2023;105:1815–1821. - PubMed
-
- Provencher M.T., Bhatia S., Ghodadra N.S., et al. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am. 2010;92:133–151. (suppl 2) - PubMed
-
- Piasecki D.P., Verma N.N., Romeo A.A., Levine W.N., Bach B.R., Provencher M.T. Glenoid bone deficiency in recurrent anterior shoulder instability: Diagnosis and management. J Am Acad Orthop Surg. 2009;17:482–493. - PubMed
-
- Porcellini G., Campi F., Paladini P. Arthroscopic approach to the bony Bankart lesion. Arthroscopy. 2002;18:764–769. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
