

Identification and validation of the fibrosis-related molecular subtypes of hepatocellular carcinoma by bioinformatics
- PMID: 40549259
- PMCID: PMC12185811
- DOI: 10.1007/s12672-025-02964-8
Identification and validation of the fibrosis-related molecular subtypes of hepatocellular carcinoma by bioinformatics
Abstract
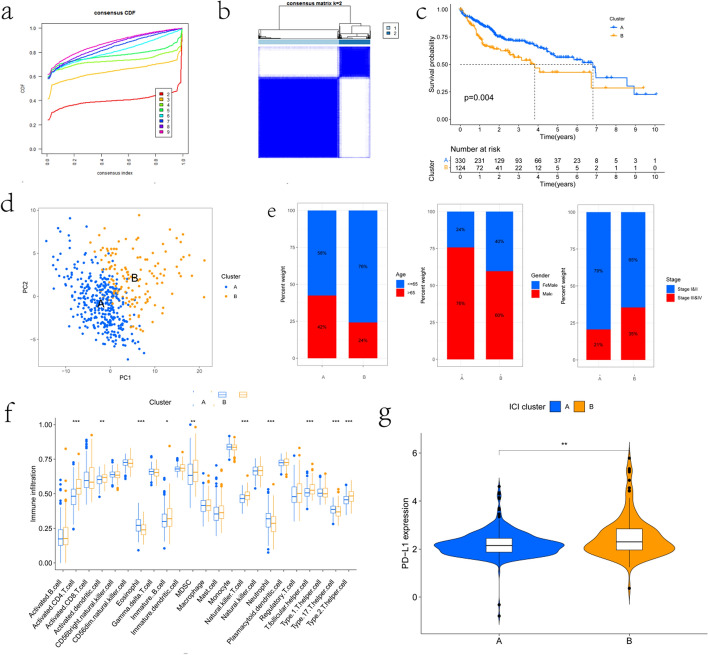
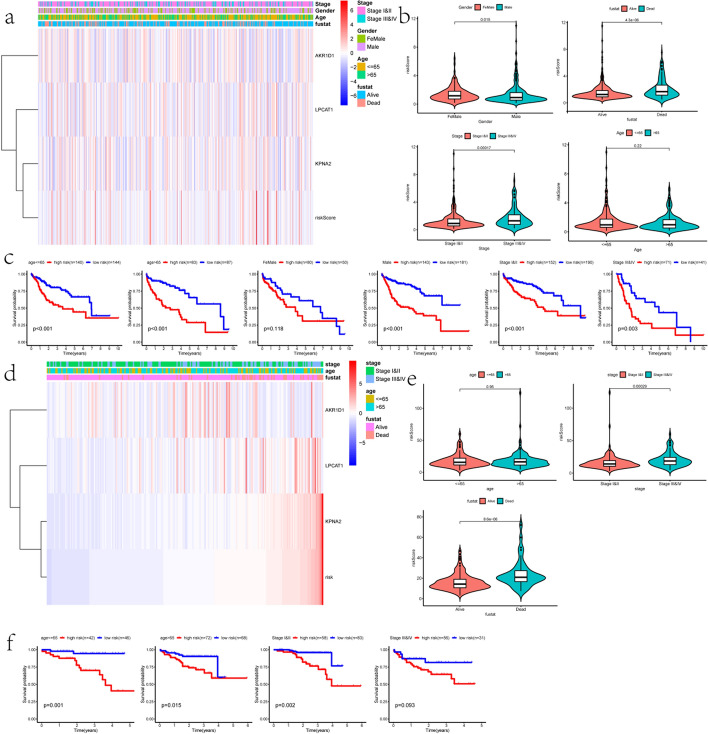
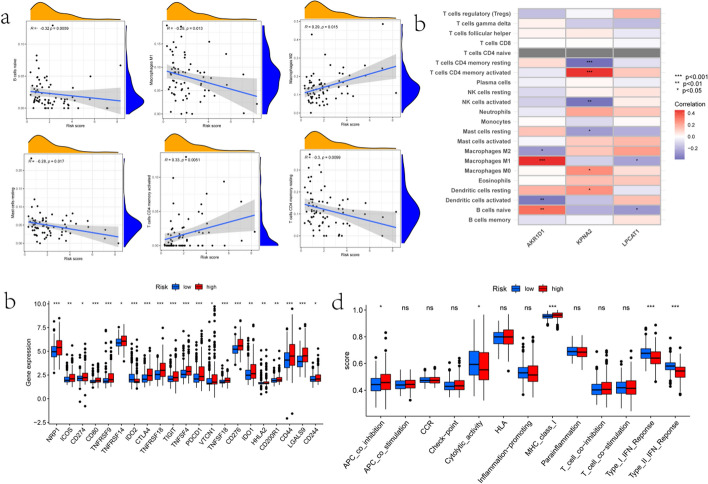
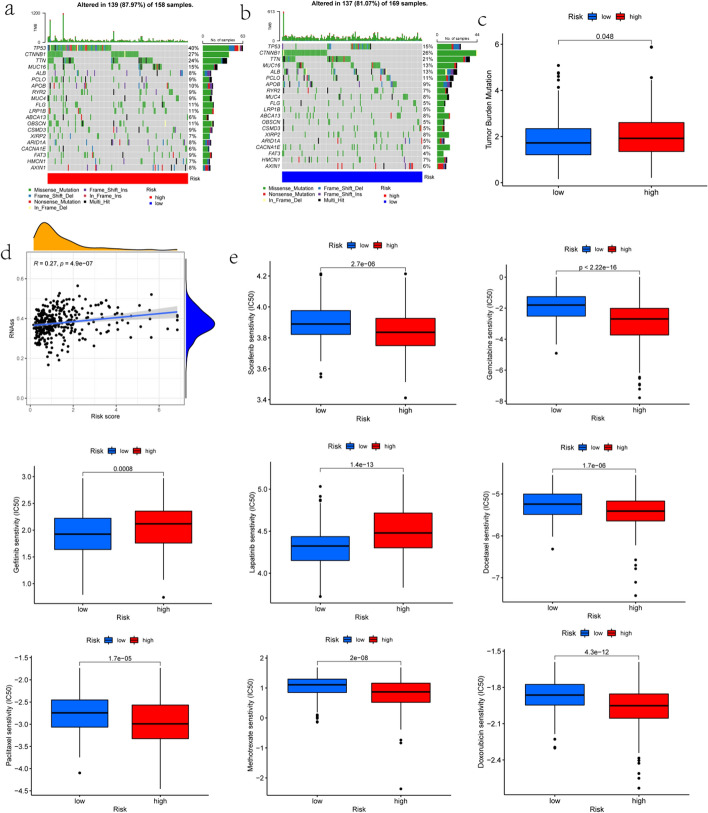
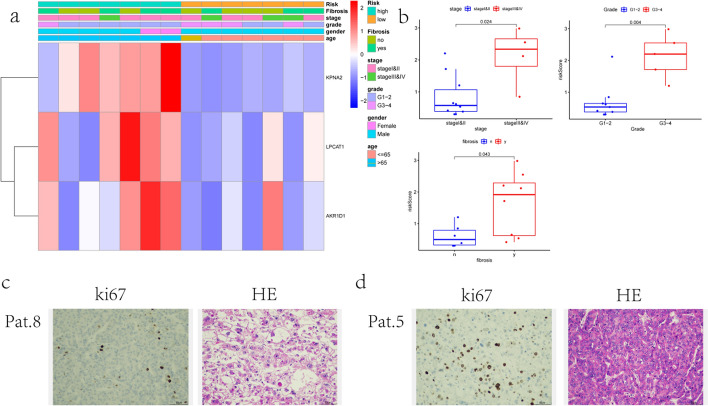
We identified novel Molecular subtypes according to the expression of fibrosis-related genes (FRGs) and constructed a prognostic model using different expression genes (DEGs) for patients with Hepatocellular carcinoma (HCC). We downloaded the clinical data and transcriptome data of HCC from The Cancer Genome Atlas (TCGA) database, Gene Expression Omnibus (GEO) database, and International Cancer Genome Consortium (ICGC) database. We identified two fibrosis-related molecular subtypes of HCC by consensus unsupervised clustering analysis. Interestingly, these two molecular subtypes significantly differed in overall survival (OS) and clinical characteristics. Besides, the most minor absolute shrinkage and selection operator (Lasso) and multivariate Cox regression analysis were performed to develop a novel prognostic model by three genes (including KPNA2, LPCAT1, and AKR1D1). There was a statistically significant difference in OS between the high-risk and low-risk groups. The area under the ROC curve (AUC) of OS in 1-, 3-, and 5-year were satisfactory. Besides, the risk score was connected with critical clinical characteristics and could be an independent factor in predicting prognosis. Then, the nomogram was built by incorporating risk scores with clinical parameters. Additionally, the risk score was remarkedly correlated with TME and drug susceptibility. Finally, the results of H&E staining and immunohistochemistry of Ki67 showed that the tumor of higher-risk patients are more malignant. The FRGs-based subtype and signature explain the HCC heterogeneity, which might provide a new method to develop a more efficient treatment.
Keywords: Drug susceptibility; Fibrosis; HCC; Immunotherapy; Prognosis model.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: This study was approved by the ethical committee of the University of Health and Rehabilitation Sciences (Qingdao Municipal Hospital) (No. 104), which was conducted in compliance with the guidelines of the Declaration of Helsinki. All participants provided written informed consent to participate in this study. Consent for publication: The authors give consent for publication of the manuscript. Competing interests: A full disclosure of all potential conflicts of interest, both financial and non-financial, has been made to uphold transparency and compliance with the journal’s ethical standards.
Figures



Similar articles
-
The molecular sub-type and the development and validation of a prognosis prediction model based on endocytosis-related genes for hepatocellular carcinoma.J Gastrointest Oncol. 2025 Jun 30;16(3):1115-1126. doi: 10.21037/jgo-2025-359. Epub 2025 Jun 27. J Gastrointest Oncol. 2025. PMID: 40672080 Free PMC article.
-
Bioinformatics identification of key microRNA-correlated genes associated with hepatocellular carcinoma heterogeneity and prognosis.BMC Gastroenterol. 2025 Jul 1;25(1):452. doi: 10.1186/s12876-025-04031-6. BMC Gastroenterol. 2025. PMID: 40596892 Free PMC article.
-
Identifying the predictive role and the related drugs of oxidative stress genes in the hepatocellular carcinoma.Cancer Rep (Hoboken). 2024 Apr;7(4):e1978. doi: 10.1002/cnr2.1978. Cancer Rep (Hoboken). 2024. PMID: 38599581 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Sung H, Ferlay J, Siegel R L et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021. - PubMed
-
- Ryu T, Takami Y, Wada Y, Hara T, Sasaki S, Saitsu H. Actual 10-year survival after surgical microwave ablation for hepatocellular carcinoma: a single center experience in Japan. Ann Surg Oncol. 2019;26(12):4126–33. - PubMed
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301–14. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous