

Surgical resection of vascular-invasive late-stage hepatocellular carcinoma following transarterial chemoembolization combined with lenvatinib and tislelizumab: Two case reports and literature review
- PMID: 40550061
- PMCID: PMC12187305
- DOI: 10.1097/MD.0000000000042973
Surgical resection of vascular-invasive late-stage hepatocellular carcinoma following transarterial chemoembolization combined with lenvatinib and tislelizumab: Two case reports and literature review
Abstract
Rationale: Hepatocellular carcinoma (HCC) with hepatic vein invasion poses significant treatment challenges and is associated with poor prognosis. Recent studies suggest that a combination of transarterial chemoembolization (TACE), targeted therapy, and immunotherapy may downstage advanced tumors, making surgical resection possible.
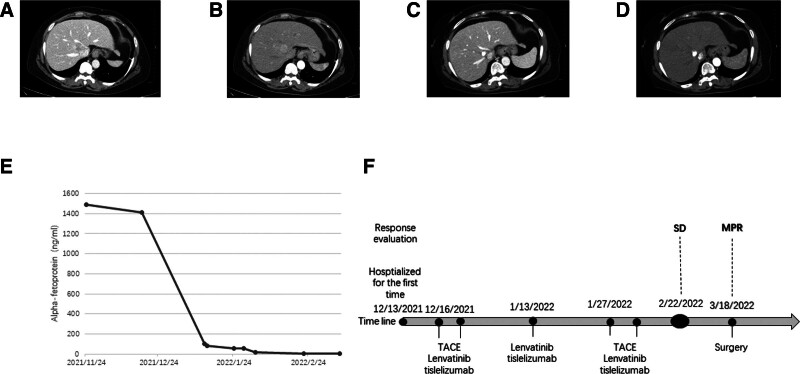
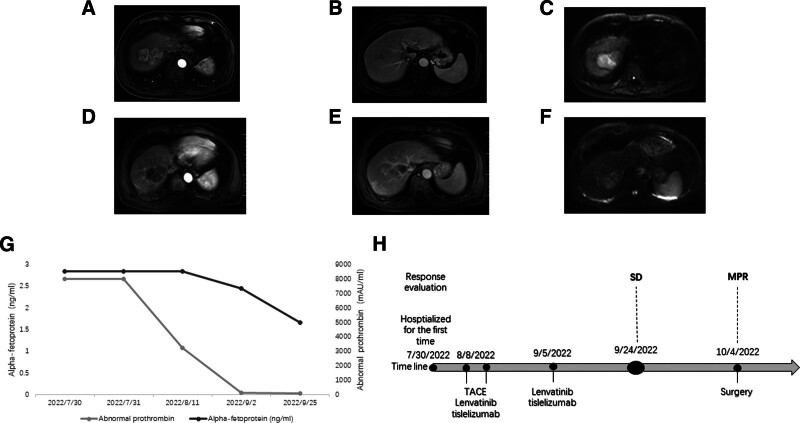
Patient concerns: A 61-year-old female presented with a 3.7 × 3.1 cm hepatic mass invading the hepatic veins. A 75-year-old male exhibited a 6.7 × 5.1 cm liver tumor involving the right hepatic vein.
Diagnoses: Both patients were diagnosed with advanced HCC with vascular invasion, confirmed by contrast-enhanced imaging and elevated alpha-fetoprotein (AFP) levels.
Interventions: In case 1, the patient received 2 rounds of TACE and 3 cycles of lenvatinib plus tislelizumab. In case 2, the patient underwent 1 TACE session and 2 cycles of the same combination therapy. Both cases showed significant tumor shrinkage, allowing subsequent R0 surgical resection.
Outcomes: Pathological evaluation following surgery revealed a major pathological response in both patients. Postoperative recovery was uneventful, and both patients remained disease-free during follow-up.
Lessons: The combination of TACE, lenvatinib, and tislelizumab may offer an effective multimodal strategy for converting unresectable HCC with vascular invasion into resectable disease, potentially improving long-term outcomes.
Keywords: HCC; TACE; gallbladder; hepatic vein; immunohistochemistry; immunotherapy; lenvatinib; liver metastasis.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Sintilimab plus lenvatinib in combination with transarterial chemoembolization and subsequent radiofrequency ablation for unresectable hepatocellular carcinoma: a single-arm, single-center study.Sci Rep. 2025 Jul 25;15(1):27123. doi: 10.1038/s41598-025-12858-y. Sci Rep. 2025. PMID: 40715509 Free PMC article.
-
Adjuvant transarterial chemoembolization plus lenvatinib for patients with HCC with MVI after resection: a multicenter retrospective study.Oncologist. 2025 Jun 4;30(6):oyaf139. doi: 10.1093/oncolo/oyaf139. Oncologist. 2025. PMID: 40504548 Free PMC article.
-
Case Report: Durable complete response of advanced-stage hepatocellular carcinoma to DEB-TACE combined with lenvatinib and camrelizumab.Front Immunol. 2025 Jun 20;16:1549675. doi: 10.3389/fimmu.2025.1549675. eCollection 2025. Front Immunol. 2025. PMID: 40621454 Free PMC article.
-
Hepatic resection alone versus in combination with pre- and post-operative transarterial chemoembolization for the treatment of hepatocellular carcinoma: A systematic review and meta-analysis.Oncotarget. 2015 Nov 3;6(34):36838-59. doi: 10.18632/oncotarget.5426. Oncotarget. 2015. PMID: 26451613 Free PMC article.
-
Clinical efficacy of lenvatinib, trans-arterial chemoembolization, and PD-1/L1 inhibitors in advanced hepatocellular carcinoma: a systematic review and network meta-analysis.Clin Transl Oncol. 2024 Oct;26(10):2652-2664. doi: 10.1007/s12094-024-03458-9. Epub 2024 Apr 26. Clin Transl Oncol. 2024. PMID: 38671328
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–49. - PubMed
-
- Lyu N, Kong Y, Mu L, et al. Hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced hepatocellular carcinoma. J Hepatol. 2018;69:60–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
