

Complete remission of peritoneal strumosis from struma ovarii after radioiodine therapy: a case report
- PMID: 40551138
- PMCID: PMC12186374
- DOI: 10.1186/s13044-025-00247-6
Complete remission of peritoneal strumosis from struma ovarii after radioiodine therapy: a case report
Abstract
Background: Struma ovarii (SO) is a specialized monodermal teratoma composed predominantly of thyroid tissue (≥ 50%) and accounts for approximately 5% of all ovarian teratomas. In rare cases, the benign SO may spread to the peritoneal cavity and exhibit the histological features of struma ovarii in a condition termed peritoneal strumosis. Here, we present a rare case of complete remission of peritoneal strumosis from SO after radioiodine therapy.
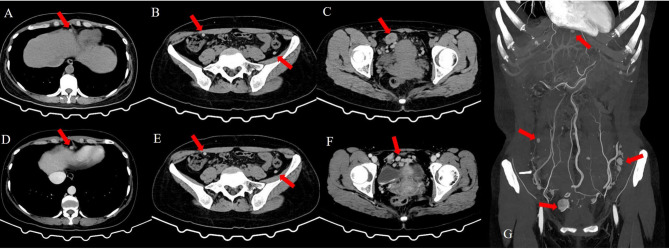
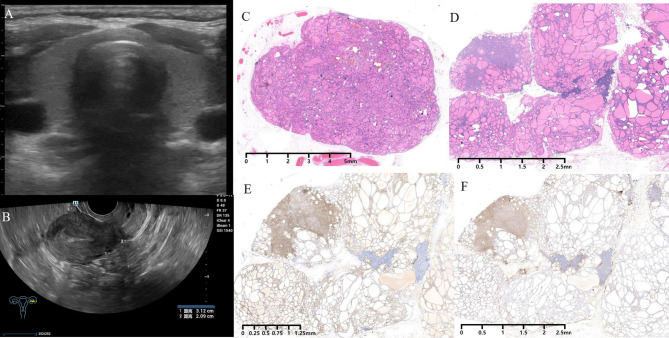
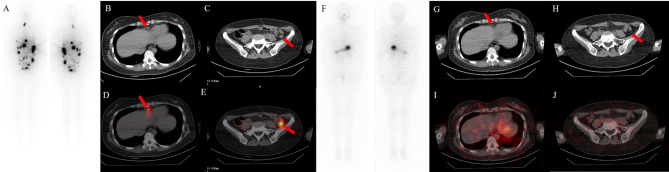
Case presentation: A 41-year-old Chinese woman underwent transabdominal left oophorectomy for a benign SO 18 years prior to presentation in the clinic. She was admitted to our institution for periodic medical examination after ultrasonography revealed a left pelvic mass. The patient underwent total abdominal hysterectomy, right salpingo-oophorectomy, and omentectomy, and multiple biopsies were taken from the omentum and mesentery. Pathology revealed peritoneal strumosis without evidence of malignancy from SO. Afterward, a total thyroidectomy was performed, and a histological examination revealed multinodular goiter. In total, 4400 MBq of 131I was administered, and lesion remission was confirmed. Finally, after 1 year of follow-up, the patient had no evidence of recurrence.
Conclusion: Peritoneal strumosis from OS is a rare aggressive clinical manifestation that differs from malignancy. Conservative surgery with personalized radioiodine may be a practical therapeutic option for unresectable peritoneal strumosis, and long-term monitoring is recommended.
Keywords: Peritoneal strumosis; Radioiodine; Struma ovarii.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This work was carried out in accordance with the Helsinki Declaration and approved by the Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (IIT-20250211 A). Consent for publication: Written informed consent to publish has been obtained from the patient. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Thyroid papillary cancer elements arising from struma ovarii with benign peritoneal strumosis: Utility of iodine-123 imaging in diagnostics and treatment planning.Clin Case Rep. 2023 May 4;11(5):e7311. doi: 10.1002/ccr3.7311. eCollection 2023 May. Clin Case Rep. 2023. PMID: 37151955 Free PMC article.
-
Successful Management and Long-term Survival of Malignant Struma Ovarii with Radioactive Iodine Therapy.Indian J Nucl Med. 2025 Mar-Apr;40(2):109-112. doi: 10.4103/ijnm.ijnm_4_25. Epub 2025 Jun 27. Indian J Nucl Med. 2025. PMID: 40735755 Free PMC article.
-
Struma ovarii and peritoneal strumosis with thyrotoxicosis.Thyroid. 2009 Mar;19(3):305-8. doi: 10.1089/thy.2008.0307. Thyroid. 2009. PMID: 19265502
-
Risk-reducing bilateral salpingo-oophorectomy in women with BRCA1 or BRCA2 mutations.Cochrane Database Syst Rev. 2018 Aug 24;8(8):CD012464. doi: 10.1002/14651858.CD012464.pub2. Cochrane Database Syst Rev. 2018. PMID: 30141832 Free PMC article.
-
Lamotrigine versus carbamazepine monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2018 Jun 28;6(6):CD001031. doi: 10.1002/14651858.CD001031.pub4. Cochrane Database Syst Rev. 2018. PMID: 29952431 Free PMC article.
References
LinkOut - more resources
Full Text Sources
