

Success of airway management in out-of-hospital cardiac arrest using different devices - a prospective, single-center, observational study comparing professions
- PMID: 40551144
- PMCID: PMC12183896
- DOI: 10.1186/s13049-025-01422-2
Success of airway management in out-of-hospital cardiac arrest using different devices - a prospective, single-center, observational study comparing professions
Abstract
Background: Endotracheal intubation is the gold standard for airway management in out-of-hospital cardiopulmonary resuscitation (CPR) but requires practice, especially in difficult conditions. To facilitate this, video laryngoscopy (VL) is increasingly used. The extent to which it is actually used in practice by paramedics or emergency physicians (EPs) and its effectiveness remain unclear. This prospective observational study investigates these aspects.
Methods: From January 2020 to June 2024, we surveyed emergency physicians and paramedics in a German county about out-of-hospital resuscitations. The questionnaire covered qualifications, airway devices, attempts, and complications. Data was analyzed descriptively and statistically. The significance level was set at alpha ≤ 0.05.
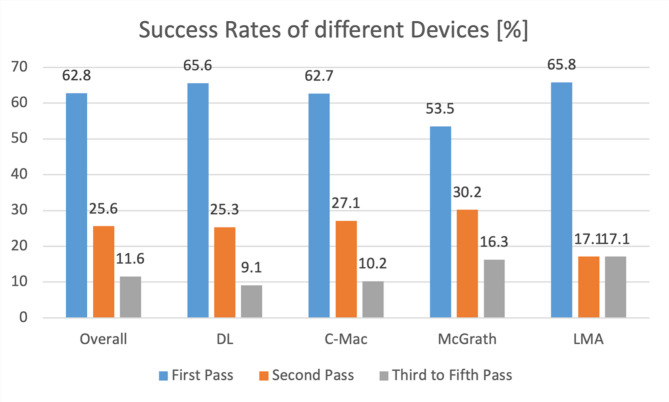
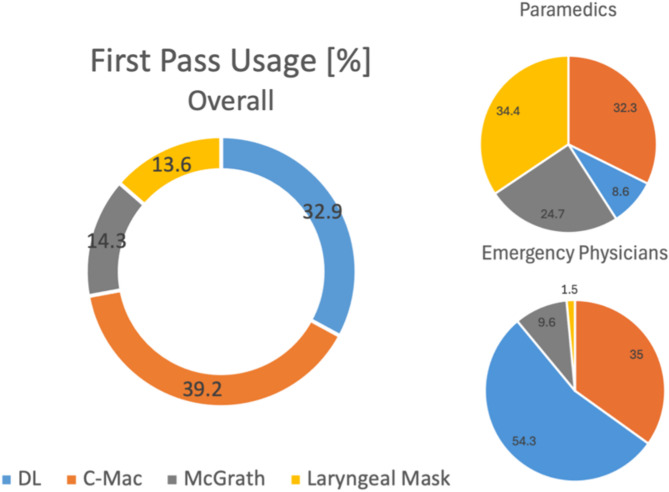
Results: 301 questionnaires were analyzed, with an overall first pass success (FPS) rate of 62.8%. No significant difference was found between direct laryngoscopy (DL) and video laryngoscopy (VL), though VL with McGrath performed worse than DL and VL with C-Mac. FPS rates did not differ significantly between emergency physicians and paramedics. Both achieved better results with their regularly used device. Paramedics used laryngeal masks more frequently (34% vs. 1.5%, p < 0.001). Among emergency physicians, anesthetists had the lowest FPS using DL (p < 0.001).
Interpretation: The FPS rate did not differ between DL and VL but was low overall. This low rate, as well as the fact that emergency physicians and paramedics achieved comparable results in intubation, might indicate an increased need for training and further education in the area of airway management for emergency personnel. However, it can also be questioned to what extent ETI can be recommended at all, with supraglottic devices being an alternative. A possible benefit of more training can be seen in the higher success rates with the more frequently used devices in both professions. An uncertainty of paramedics regarding endotracheal intubation is also reflected in an more frequent use of laryngeal masks. The fact that internists who used VL more frequently had better FPS rates than anesthetists who intubated conventionally more often shows the potential of VL, especially under difficult out-of-hospital intubation conditions.
Trial registration: The study was registered in the German Clinical Trials Register (DRKS ID: DRKS00021821, 12.06.2020).
Keywords: Airway management; Emergency medical services; Endotracheal intubation; Out-of-hospital cardiac arrest; Video laryngoscopy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Positive vote of the ethics board of the Philipps University of Marburg, Germany from 02/09/2019 (Ethics Committee processing number: 134/19). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation.Cochrane Database Syst Rev. 2016 Nov 15;11(11):CD011136. doi: 10.1002/14651858.CD011136.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2022 Apr 4;4:CD011136. doi: 10.1002/14651858.CD011136.pub3. PMID: 27844477 Free PMC article. Updated.
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation.Cochrane Database Syst Rev. 2022 Apr 4;4(4):CD011136. doi: 10.1002/14651858.CD011136.pub3. Cochrane Database Syst Rev. 2022. PMID: 35373840 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Fischer M, Wnent J, Gräsner J-T, Seewald S, Rück L, Hoffmann H, Bein B, Ramshorn-Zimmer A, Bohn A. & Die teilnehmenden rettungsdienste im, Deutschen reanimationsregister. Öffentlicher Jahresbericht 2023 des Deutschen Reanimationsregisters: Außerklinische Reanimation 2023 [Internet]. 2024. Verfügbar unter: https://www.reanimationsregister.de/downloads/oeffentliche-jahresbericht...
-
- Hasegawa K, Shigemitsu K, Hagiwara Y, Chiba T, Watase H, Brown CA. u. A. Association between repeated intubation attempts A.d adverse events in emergency departments: an analysis of A.Multicenter prospective observational study. Ann Emerg Med Dezember. 2012;60(6):749–e7542. - PubMed
-
- Mort TC. Complications of emergency tracheal intubation: hemodynamic Alterations - Part I. J Intensive Care Med Mai. 2007;22(3):157–65. - PubMed
-
- Murphy DL, Bulger NE, Harrington BM, Skerchak JA, Counts CR, Latimer AJ. u. A. Fewer tracheal intubation A.tempts A.e A.sociated with improved neurologically intact survival following out-of-hospital cardiac A.rest. Resusc Oktober. 2021;167:289–96. - PubMed
-
- Timmermann A. S1-Leitlinie: prähospitales atemwegsmanagement (Kurzfassung). Timmermann böttiger BW Byhahn C Dörges V Eich C Gräsner JT al S1-Leitlin prähospitales atemwegsmanagement Kurzfass. 7 Juni 2019;(6–2019):316–36.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
