

Dexmedetomidine-enhanced chest wall fascial plane blocks in ultra-fast-track minimally invasive heart valve surgery: a randomized controlled trial
- PMID: 40551199
- PMCID: PMC12183839
- DOI: 10.1186/s13741-025-00547-3
Dexmedetomidine-enhanced chest wall fascial plane blocks in ultra-fast-track minimally invasive heart valve surgery: a randomized controlled trial
Abstract
Background: Injury to the sternocostal joint during minimally invasive cardiac surgery frequently results in severe pain, yet there is no established standard for perioperative analgesia. This randomized controlled trial evaluated whether adding 1 μg/kg dexmedetomidine to 0.375% ropivacaine for chest wall fascial plane blocks enhances opioid sparing in ultra-fast-track (UFT) minimally invasive heart valve surgery.
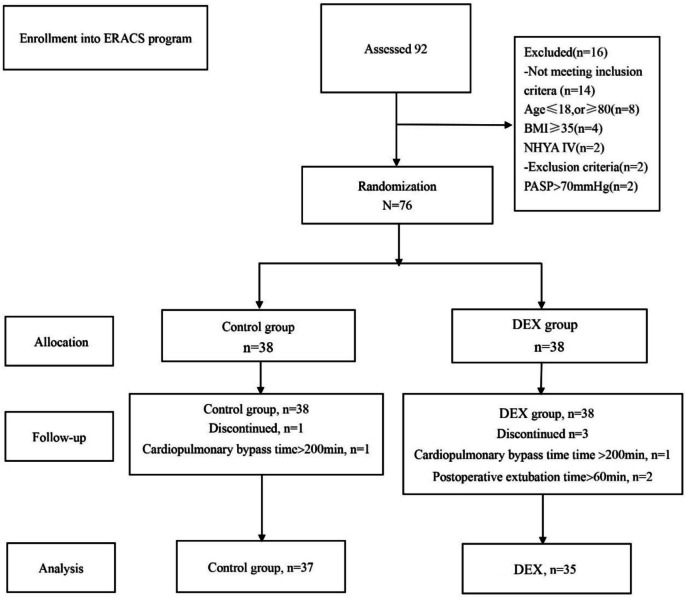
Methods: Seventy-six elective patients were randomized (1:1) in a double-blind manner. The control group received 60 mL of 0.375% ropivacaine, while the DEX group was administered 60 mL of 1 μg/kg dexmedetomidine plus 0.375% ropivacaine. The primary outcomes were intraoperative remifentanil use and 24-h postoperative sufentanil consumption, which served as co-primary endpoints to evaluate opioid-sparing effects. Secondary outcomes included 24-h postoperative sufentanil consumption, 24-h oxycodone use, patient-controlled analgesia (PCA) activations, episodes of Visual Analog Scale (VAS) scores ≥ 3 within 48 h, time to recovery of consciousness, time to extubation, duration of intensive care unit (ICU), and hospital stays, and complications.
Results: The DEX group exhibited significantly reduced intraoperative remifentanil consumption (2.45 ± 0.47 vs. 2.98 ± 0.53 mg, p < 0.001) and 24-h sufentanil use (median with interquartile range (IQR) 57 [54-60] vs. 63 [63-66] μg, p < 0.001). It also demonstrated lower 24-h oxycodone consumption (median [IQR] 5 [0-10] vs. 10 [10-20] mg, p < 0.001), fewer 24-h PCA activations (median [IQR] 3 [2-4] vs. 5 [5-6], p < 0.001), and less frequent VAS ≥ 3 episodes (median [IQR] 3 [2.5-4] vs. 6 [5-6], p < 0.001), alongside shorter lengths of ICU (21.34 ± 3.59 vs. 24.29 ± 4.07 h, p = 0.002) and hospital stays (6.51 ± 1.04 vs. 8.65 ± 1.80 days, p < 0.001). Postoperative complications did not differ significantly between groups, though dexmedetomidine-related hemodynamic effects were not systematically monitored.
Conclusion: The administration of 1 μg/kg dexmedetomidine in combination with ropivacaine for chest wall fascial plane blocks reduces opioid requirements and shortens ICU/hospital stays in UFT cardiac surgery, supporting its safety and efficacy, but limitations include the single-center design, fixed dexmedetomidine dosage, and incomplete complication assessment, warranting multicenter validation with standardized safety monitoring.
Trial registration: ChiCTR2100051182.
Keywords: Dexmedetomidine; Chest wall fascial plane block; Ultra-fast-track; Minimally invasive heart valve surgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Ethics Committee of Zhejiang Provincial People’s Hospital approved this study. All study participants provided written informed consent for participation. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Safety and efficacy of low-dose esketamine weakly opioidized anesthesia in elderly patients with lumbar spinal stenosis undergoing surgery: a prospective, double-blind randomized controlled trial.BMC Anesthesiol. 2025 Feb 5;25(1):57. doi: 10.1186/s12871-025-02908-3. BMC Anesthesiol. 2025. PMID: 39910473 Free PMC article. Clinical Trial.
-
Limited versus full sternotomy for aortic valve replacement.Cochrane Database Syst Rev. 2017 Apr 10;4(4):CD011793. doi: 10.1002/14651858.CD011793.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Dec 6;12:CD011793. doi: 10.1002/14651858.CD011793.pub3. PMID: 28394022 Free PMC article. Updated.
-
Efficacy of opioid-free anesthesia in reducing postoperative nausea and vomiting following gynecological laparoscopic surgery: a randomized controlled trial.Front Med (Lausanne). 2025 Jul 17;12:1606383. doi: 10.3389/fmed.2025.1606383. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40747089 Free PMC article.
-
Dexamethasone and dexmedetomidine as adjuvants to local anesthetic mixture in erector spinae plane block combined with serratus anterior plane block for thoracoscopic surgery: a prospective, randomized controlled trial.Minerva Anestesiol. 2025 Jun 23. doi: 10.23736/S0375-9393.25.18895-0. Online ahead of print. Minerva Anestesiol. 2025. PMID: 40548617
-
Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults.Cochrane Database Syst Rev. 2018 Jun 4;6(6):CD009642. doi: 10.1002/14651858.CD009642.pub3. Cochrane Database Syst Rev. 2018. PMID: 29864216 Free PMC article.
References
-
- Barr LF, Boss MJ, Mazzeffi MA, Taylor BS, Salenger R. Postoperative multimodal analgesia in cardiac surgery. Crit Care Clin. 2020;36:631–51. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
