

Multiple-breath washout is more sensitive than spirometry to detect lung function impairment in children and adults with bronchiectasis
- PMID: 40551806
- PMCID: PMC12183715
- DOI: 10.1183/23120541.00987-2024
Multiple-breath washout is more sensitive than spirometry to detect lung function impairment in children and adults with bronchiectasis
Abstract
Background: Multiple-breath washout (MBW) is an established outcome measure of lung disease in cystic fibrosis (CF). However, data on its sensitivity to detect lung function impairment in bronchiectasis across age groups remain limited. The aim of this study was therefore to determine the feasibility, validity and sensitivity of MBW compared with spirometry in people with bronchiectasis.
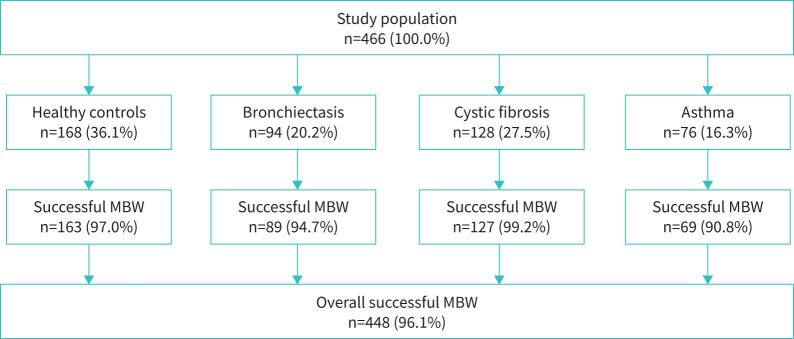
Methods: We performed MBW and spirometry in 94 people with bronchiectasis (aged 0.2 to 79.3 years), 168 healthy controls, and 128 people with CF and 76 with asthma as disease controls.
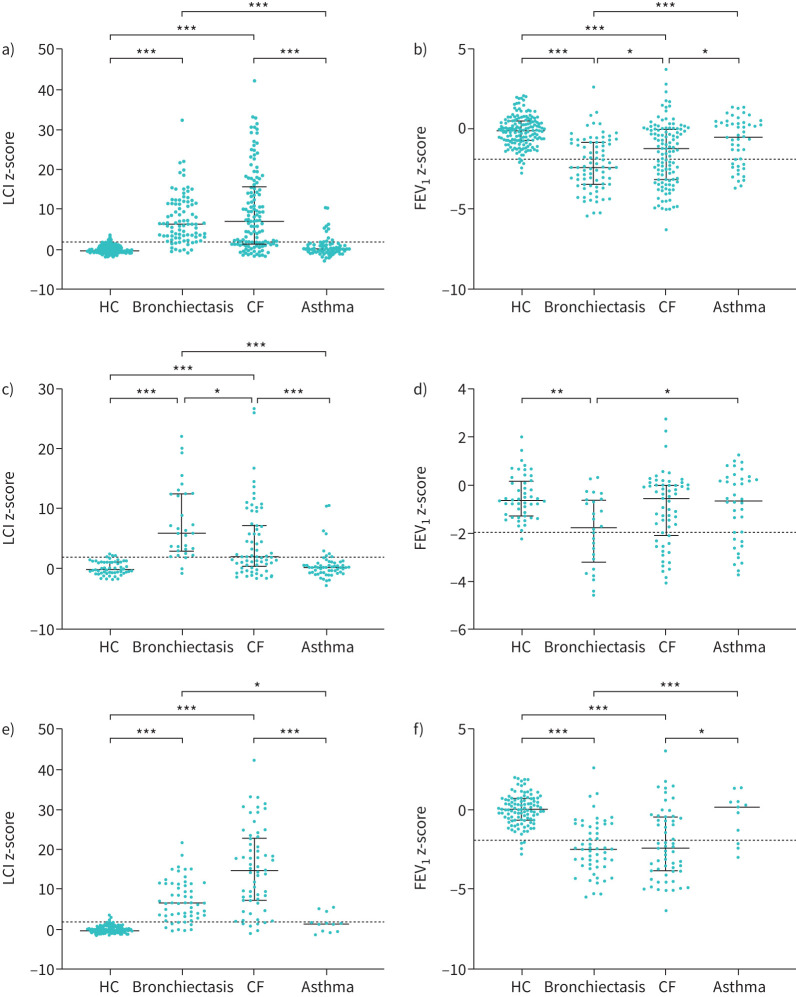
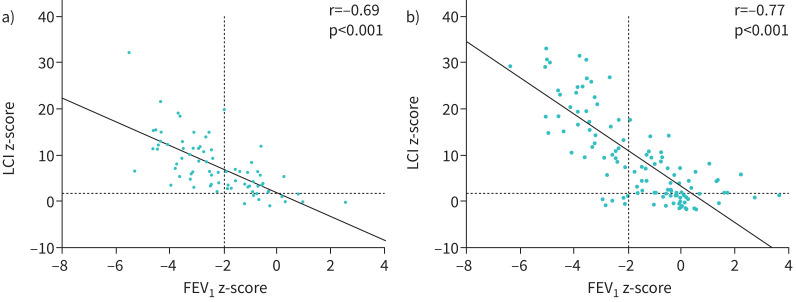
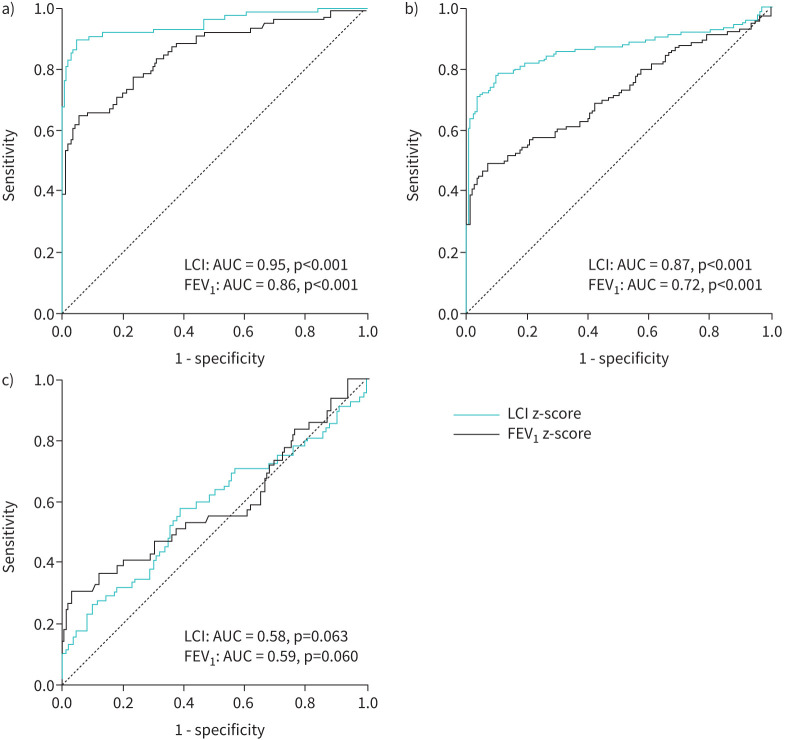
Results: The overall success rate of MBW in all 466 participants was 96.1%. People with bronchiectasis had an elevated lung clearance index (LCI) and a reduced forced expiratory volume in 1 s (FEV1) compared with healthy controls and people with asthma (all p<0.001). Comparing bronchiectasis and CF, there was no difference in LCI, but FEV1 was reduced in bronchiectasis (p=0.032). Within the bronchiectasis group, LCI correlated strongly with FEV1 (r= -0.69, p<0.001). However, 34.3% of people with bronchiectasis presented with an elevated LCI but normal FEV1, while none had a reduced FEV1 combined with a normal LCI (p<0.001). LCI was superior to FEV1 in detecting lung function impairment in bronchiectasis (area under the curve: 0.95 versus 0.86).
Conclusion: LCI is more sensitive than FEV1 to detect lung function impairment in bronchiectasis. These findings support further evaluation of LCI for clinical monitoring and as a sensitive outcome measure in clinical trials in people with bronchiectasis.
Copyright ©The authors 2025.
Conflict of interest statement
Conflict of interest: J.F. Roehmel reports lecture honoraria from Vertex Pharmaceuticals outside of the submitted work. M.A. Mall reports grants from the German Research Foundation (DFG), the German Ministry for Education and Research (BMBF), the German Innovation Fund, Vertex Pharmaceuticals and Boehringer Ingelheim; consulting fees from Abbvie, Boehringer Ingelheim, Enterprise Therapeutics, Kither Biotech, Prieris, Recode, Splisense and Vertex Pharmaceuticals; lecture honoraria from Vertex Pharmaceuticals; travel support from Boehringer Ingelheim and Vertex Pharmaceuticals; advisory board participation with Abbvie, Boehringer Ingelheim, Enterprise Therapeutics, Kither Biotech, Pari and Vertex Pharmaceuticals outside the submitted work; and is Fellow of ERS. M. Stahl reports an Independent Research Innovation Award and honoraria for lectures and participation in advisory boards, all by Vertex Pharmaceuticals Incorporated, outside of the submitted work. She is Chairman of the German CF Research Council (FGM), Treasurer of the German Society of Paediatric Pulmonology (GPP), and was Secretary of the Group CF of the Paediatric Assembly of ERS. All other authors have nothing to disclose.
Figures
References
LinkOut - more resources
Full Text Sources