

Two Cases of Small Intestinal Follicular Lymphoma Presenting with Intestinal Stricture
- PMID: 40552007
- PMCID: PMC12183004
- DOI: 10.70352/scrj.cr.25-0108
Two Cases of Small Intestinal Follicular Lymphoma Presenting with Intestinal Stricture
Abstract
Introduction: Primary gastrointestinal follicular lymphoma (FL) rarely causes intestinal stricture. We report two cases of small intestinal FL presenting with stricture.
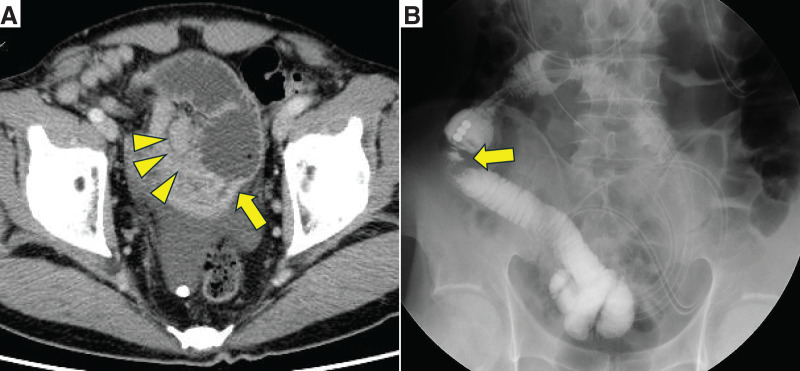
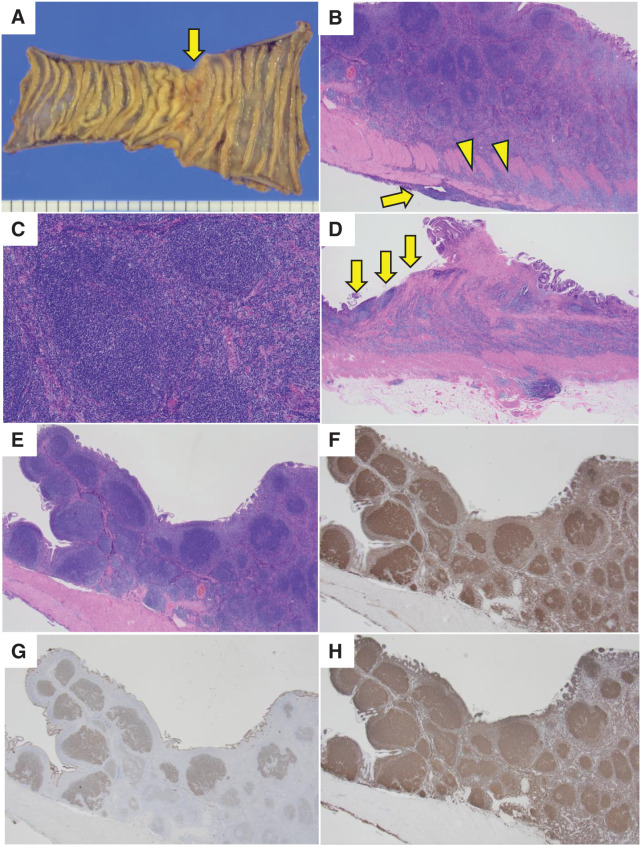
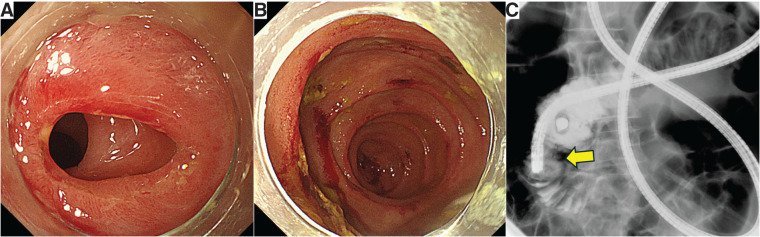
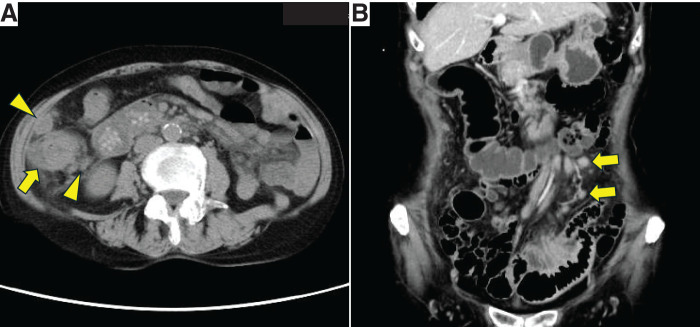
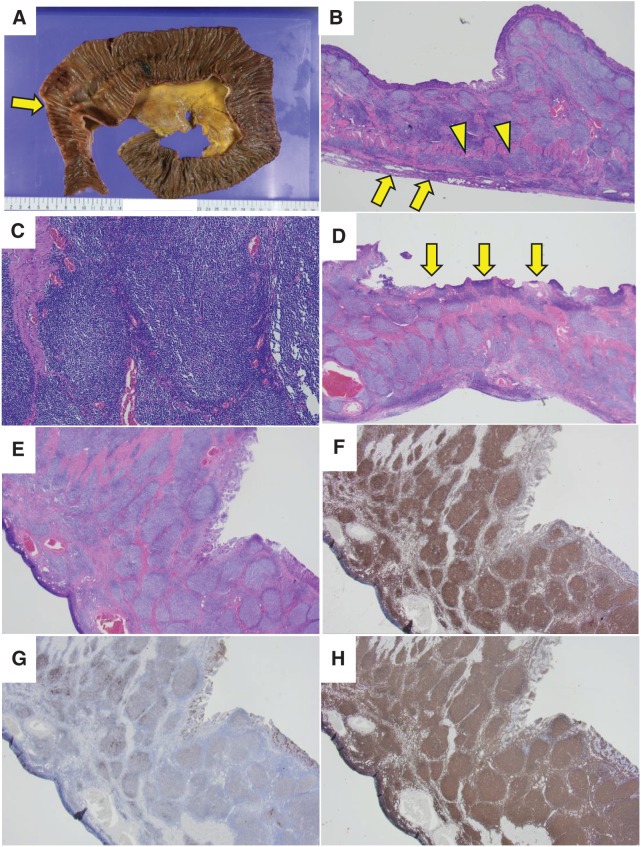
Case presentation: Case 1: A 63-year-old man presented with small intestinal obstruction. CT demonstrated ileal wall thickening and enlarged lymph nodes. Partial ileal resection confirmed primary ileal FL, immunohistochemically positive for CD10, CD20, and BCL-2. Case 2: A 79-year-old woman with a 7-year history of jejunal strictures underwent right hemicolectomy for ascending colon cancer and partial jejunal resection. Pathologic examination showed concurrent jejunal FL and colon adenocarcinoma. Immunohistochemical findings were the same as in Case 1. In both patients, postoperative positron-emission tomography-CT showed no residual lymphoma. Both were monitored clinically without chemotherapy.
Conclusions: These cases highlight an unusual presentation of follicular lymphoma as a cause of intestinal stricture. Surgical resection provided diagnostic clarity and relief of symptoms. Postoperative treatment was tailored to individual patient characteristics and residual disease status.
Keywords: follicular lymphoma; lymphoma; obstruction; small intestine; stricture.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
All authors declare no competing interests for this article.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Stem cell transplantation for induction of remission in medically refractory Crohn's disease.Cochrane Database Syst Rev. 2022 May 13;5(5):CD013070. doi: 10.1002/14651858.CD013070.pub2. Cochrane Database Syst Rev. 2022. PMID: 35556242 Free PMC article.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
A rare case report of first-trimester intestinal obstruction masquerading as ectopic pregnancy: Insights from a low-resource setting.Int J Surg Case Rep. 2025 Jul;132:111484. doi: 10.1016/j.ijscr.2025.111484. Epub 2025 Jun 7. Int J Surg Case Rep. 2025. PMID: 40499449 Free PMC article.
-
Intestinal endometriosis: A rare cause of acute care surgery.Ulus Travma Acil Cerrahi Derg. 2025 Jun;31(6):556-561. doi: 10.14744/tjtes.2025.85691. Ulus Travma Acil Cerrahi Derg. 2025. PMID: 40511762 Free PMC article.
References
-
- Li Z, Chen X, Wang Z, et al. Clinicopathologic features and prognosis analysis of gastrointestinal follicular lymphoma: a multi-center study. Front Oncol 2022; 12: 841058.
-
- Marks E, Shi Y, Grashow R, et al. Characteristics, management and outcomes of gastrointestinal follicular lymphoma: a multi-institutional study. Leuk Lymphoma 2022; 63: 2908–16.
-
- Castro-Pochintesta BA, Ruano-Ravina A, Coupland SE, et al. Endoscopic features of gastrointestinal follicular lymphoma: systematic review and meta-analysis. United European Gastroenterol J 2021;781–90.
-
- Yamamoto E, Tomita N, Sakata S, et al. Long-term outcomes of patients with primary gastrointestinal follicular lymphoma treated with rituximab-based systemic immunochemotherapy. Hematol Oncol 2023; 41:90–8.