

Cumulative Live Birth Rates in Women Undergoing Progestin-Primed Ovarian Stimulation Using Medroxyprogesterone Acetate, Dydrogesterone, and Progesterone: A Retrospective Analysis
- PMID: 40552092
- PMCID: PMC12183567
- DOI: 10.2147/DDDT.S523076
Cumulative Live Birth Rates in Women Undergoing Progestin-Primed Ovarian Stimulation Using Medroxyprogesterone Acetate, Dydrogesterone, and Progesterone: A Retrospective Analysis
Abstract
Purpose: To investigate possible differences in cumulative live birth rates (CLBRs) among three progestins medroxyprogesterone acetate (MPA), dydrogesterone (DYG), and Progesterone within the progestin-primed ovarian stimulation (PPOS) protocol.
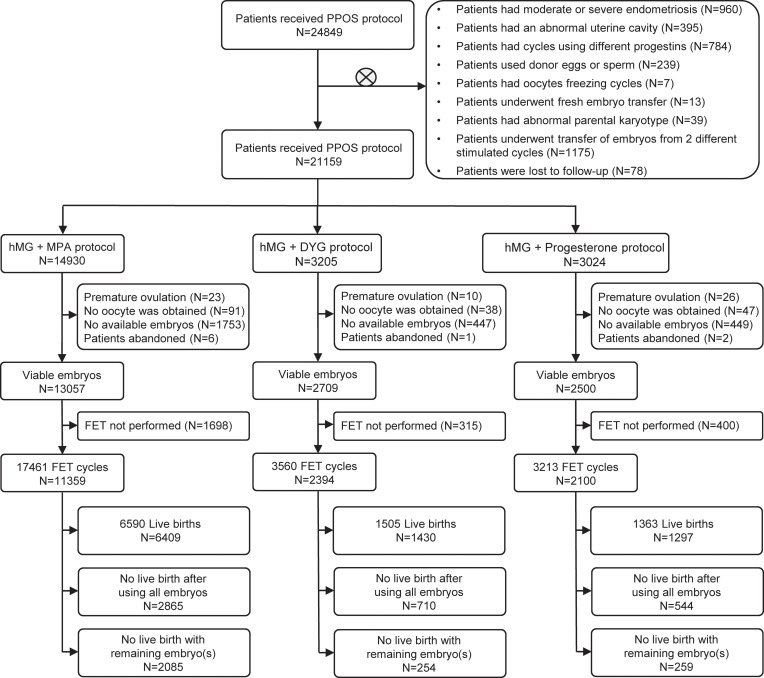
Patients and methods: This retrospective study included 21,159 women undergoing one of three ovarian stimulation protocols, hMG + MPA, hMG + DYG, or hMG + Progesterone, between September 2013 and January 2024 in our centre. Patients received oral progestins once daily as per their assigned protocol with human menopausal gonadotropin initiated on menstrual cycle day 3. The primary outcome was the CLBR. Secondary outcomes comprised ovarian stimulation parameters, pregnancy outcomes per embryo transfer, and cumulative outcomes per individual.
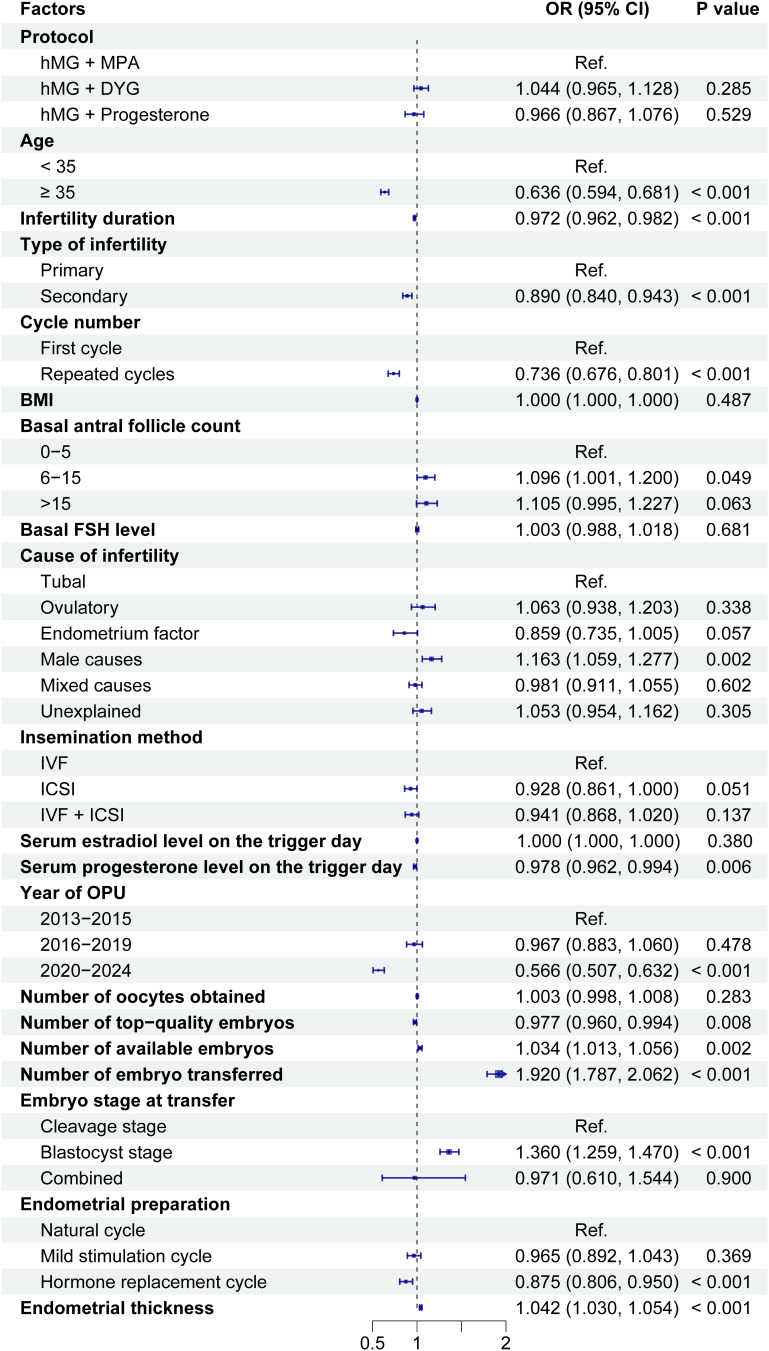
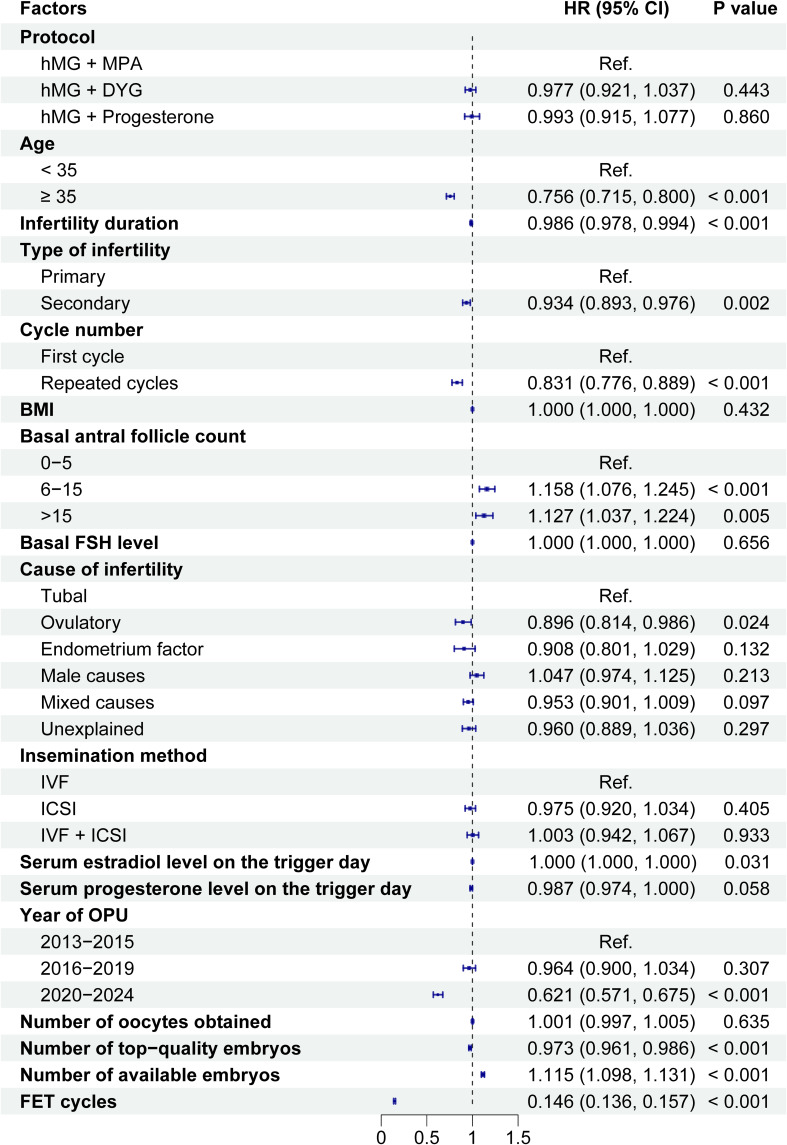
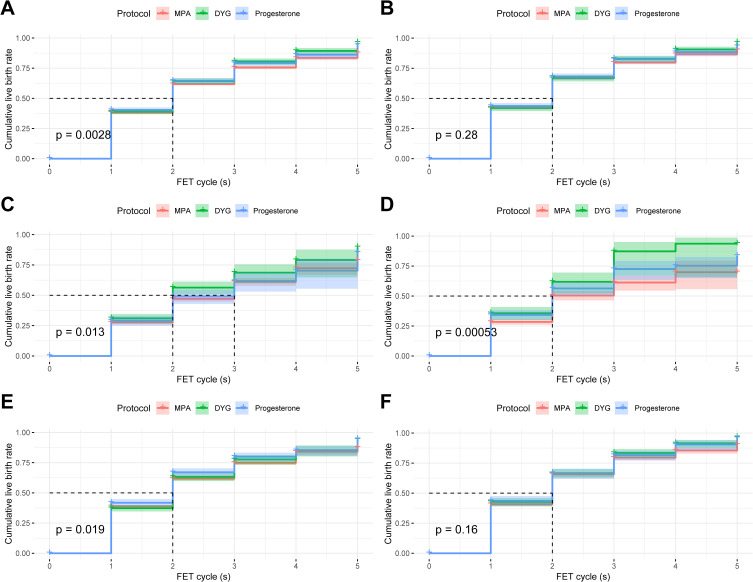
Results: The CLBR demonstrated no statistically significant differences across the three progestin regimens: MPA (6409/14,930, 42.9%), DYG (1430/3205, 44.6%), and Progesterone (1297/3024, 42.9%; p = 0.203). Kaplan-Meier analysis revealed progressive CLBR accumulation through 5 frozen-thawed embryo transfer (FET) cycles, reaching 87.6%, 95.6%, and 93.7% for MPA, DYG, and Progesterone groups, respectively, with all groups achieving 50% CLBR by the second cycle. Cox regression adjusted for confounders confirmed comparable CLBR trajectories (p > 0.05), while multivariable logistic regression showed no association between progestin type and per-cycle live birth rate (p > 0.05). Notably, the Progesterone group exhibited elevated serum progesterone levels (trigger day: p < 0.05), whereas both DYG and Progesterone groups demonstrated higher LH levels than MPA (p < 0.05).
Conclusion: Our findings establish clinical equivalence in cumulative live birth outcomes among MPA, DYG, and Progesterone when implemented within the PPOS framework. This evidence supports protocol flexibility in progestin selection, enabling personalized decisions based on pharmacological characteristics, cost considerations, and patient tolerance.
Keywords: cumulative live birth rate; dydrogesterone; frozen embryo transfer; medroxyprogesterone acetate; progesterons; progestin-primed ovarian stimulation.
© 2025 Wu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Kuang Y, Chen Q, Fu Y, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril. 2015;104(1):62–70e3. doi: 10.1016/j.fertnstert.2015.03.022 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
