

Familial hypercholesterolaemia with early-onset coronary artery disease and recurrent in-stent restenosis associated with the LDLR gene c.428G>A mutation: a case report
- PMID: 40552191
- PMCID: PMC12183192
- DOI: 10.3389/fcvm.2025.1573543
Familial hypercholesterolaemia with early-onset coronary artery disease and recurrent in-stent restenosis associated with the LDLR gene c.428G>A mutation: a case report
Abstract
Background: Familial hypercholesterolaemia (FH) is characterised by significantly elevated low-density lipoprotein cholesterol (LDL-C) levels and early-onset coronary artery disease. Additionally, clopidogrel resistance is observed in approximately 30%-50% of individuals globally. Among FH patients with early-onset coronary artery disease, inadequate LDL-C management and suboptimal antiplatelet therapy after stent implantation are key factors contributing to recurrent in-stent restenosis (ISR).
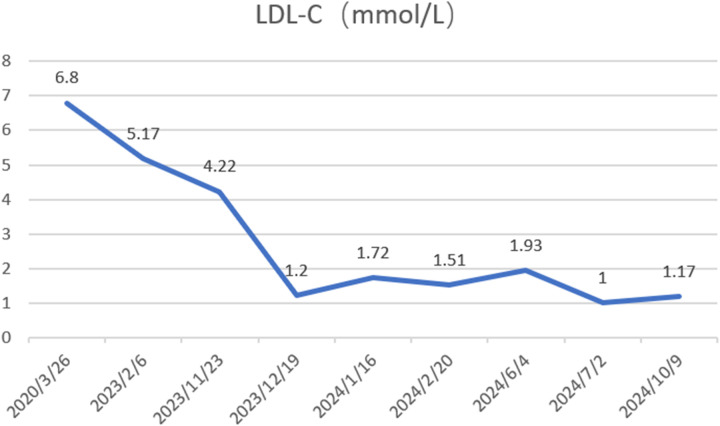
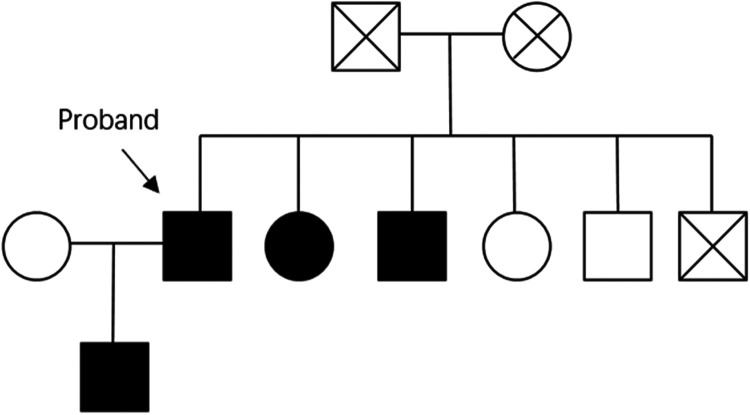
Case presentation: A 65-year-old male with a history of coronary artery disease (CAD), hyperlipidemia, and prior angioplasty presented to our institution with exacerbation of angina symptoms. The patient's CAD was initially diagnosed at age 52 (early-onset), with subsequent coronary angiography performed at Lianshui County Hospital. Coronary angiography confirmed coronary artery disease, prompting percutaneous coronary intervention (PCI) with stent placement: one in the right coronary artery and another in the left circumflex artery. Despite receiving standard antiplatelet (aspirin enteric-coated tablets 100 mg, clopidogrel 75 mg) and lipid-lowering therapy (pitavastatin calcium 2 mg), his LDL-C levels remained poorly controlled, and chest pain recurred. At the age of 62 and 65, he developed ISR with additional coronary artery lesions, necessitating balloon angioplasty. FH gene sequencing and clopidogrel resistance testing found he have a heterozygous LDL receptor (LDLR) gene mutation (c.428G>A, p.Cys143Tyr) and a clopidogrel genotype of CYP2C19 *1/*2. Based on these findings, his antiplatelet and lipid-lowering therapies were adjusted (aspirin 100 mg, clopidogrel 150 mg, rosuvastatin 10 mg, ezetimibe 10 mg and alirocumab 150 mg biweekly). Follow-up revealed that his LDL-C levels reached target values, and he remained asymptomatic. One year later, coronary angiography showed no disease progression, and the patient experienced no recurrence of chest pain. This case highlights the efficacy of precision treatment.
Conclusions: For FH patients with early-onset CAD who are intolerant to ticagrelor, early implementation of FH genetic sequencing and clopidogrel genotyping is critical for personalised treatment.
Keywords: LDL receptor gene mutation; PCSK9 inhibitors; early-onset coronary artery disease; familial hypercholesterolaemia; precision medicine; recurrent in-stent restenosis.
© 2025 Zhang, Li, Zhang, Huang and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Comparative effects of different antiplatelet strategies in carriers of CYP2C19 loss-of-function alleles: a network meta-analysis.Eur Heart J Cardiovasc Pharmacother. 2024 Oct 4;10(6):526-536. doi: 10.1093/ehjcvp/pvae036. Eur Heart J Cardiovasc Pharmacother. 2024. PMID: 38754988
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2000;4(29):1-123. Health Technol Assess. 2000. PMID: 11109029
-
Coronary artery stents: a rapid systematic review and economic evaluation.Health Technol Assess. 2004 Sep;8(35):iii-iv, 1-242. doi: 10.3310/hta8350. Health Technol Assess. 2004. PMID: 15361315
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.Health Technol Assess. 2008 May;12(21):iii, xi-xiii, 1-212. doi: 10.3310/hta12210. Health Technol Assess. 2008. PMID: 18485273
-
Dietary treatment for familial hypercholesterolaemia.Cochrane Database Syst Rev. 2001;(2):CD001918. doi: 10.1002/14651858.CD001918. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2010 Jan 20;(1):CD001918. doi: 10.1002/14651858.CD001918.pub2. PMID: 11406018 Updated.
References
-
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. (2020). 41(1):111–88. 10.1093/eurheartj/ehz455. Erratum in: Eur Heart J. (2020) 41(44):4255. doi: 10.1093/eurheartj/ehz826 - DOI - DOI - PubMed
-
- Nordestgaard BG, Chapman MJ, Humphries SE, Ginsberg HN, Masana L, Descamps OS, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease. Eur Heart J. (2013) 34(45):3478–90. 10.1093/eurheartj/eht273 - DOI - PMC - PubMed
-
- Couture P, Brun LD, Szots F, Lelièvre M, Gaudet D, Després JP, et al. Association of specific LDL receptor gene mutations with differential plasma lipoprotein response to simvastatin in young French Canadians with heterozygous familial hypercholesterolemia. Arterioscler Thromb Vasc Biol. (1998) 18(6):1007–12. 10.1161/01.atv.18.6.1007 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous