

HER2 and hormone receptor conversion after neoadjuvant therapy for breast cancer
- PMID: 40552275
- PMCID: PMC12183234
- DOI: 10.3389/fonc.2025.1522460
HER2 and hormone receptor conversion after neoadjuvant therapy for breast cancer
Abstract
Background: The expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) in residual lesions may be different compared with primary tumors of the breast after neoadjuvant therapy (NAT). Given the clinical implications of hormone receptor expression for breast cancer management, we assessed conversions in ER, PR, and HER2 in breast cancer patients after NAT.
Methods: Our study comprised 589 individuals with aggressive breast cancer who underwent NAT. We examined the ER, PR, and HER2 statuses in primary and residual breast cancers and investigated the relationship between receptor conversion and clinicopathological variables.
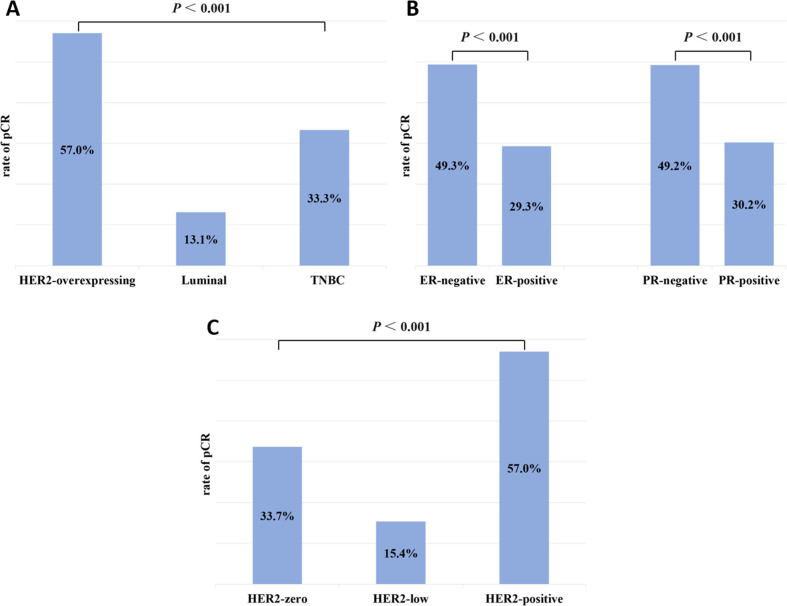
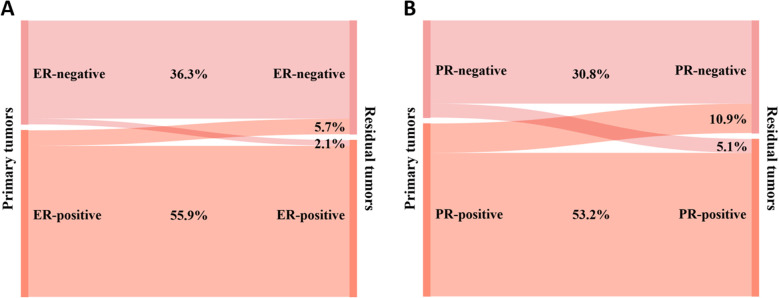
Results: The pathologic complete response (pCR) rate for the overall cohort was 38.7%, with pCR rates of 57.0%, 13.1%, and 33.3% for HER2-positive, Luminal, and triple-negative breast cancer (TNBC), respectively. Cases with negative hormone receptor expression were more likely to achieve pCR than positive cases. The highest pCR rates were seen in HER2-positive breast cancers, followed by HER2-zero and HER2-low tumors. After NAT, there were 26 (7.8%) cases of ER status conversion and 53 (16.0%) cases of PR status conversion. The conversion of hormone receptors was mainly from positive to negative. When cases were categorized as HER2-negative or positive, 15 (5.1%) cases had a conversion of HER2 status, predominantly positive to negative. When cases were classified as HER2-zero, -low, or -positive, HER2 status conversion happened in 54 (18.6%) cases and was mostly happened between HER2-zero and HER2-low. HER2 status before NAT correlated with ER and HER2 conversion.
Conclusion: Some breast cancer patients may show ER, PR, or HER2 status conversion after NAT. Residual lesions need to be immunohistochemically re-tested to reassess the patient's receptor expression status and to adjust the subsequent treatment regimen.
Keywords: breast cancer; estrogen receptor; human epidermal growth factor receptor 2; neoadjuvant therapy; progesterone receptor.
Copyright © 2025 Wang, Long, Tang and Xiao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous