

Allogenic mitochondria transfer improves cardiac function in iPS-cell-differentiated cardiomyocytes of a patient with Barth syndrome
- PMID: 40555742
- PMCID: PMC12229508
- DOI: 10.1038/s12276-025-01472-7
Allogenic mitochondria transfer improves cardiac function in iPS-cell-differentiated cardiomyocytes of a patient with Barth syndrome
Abstract
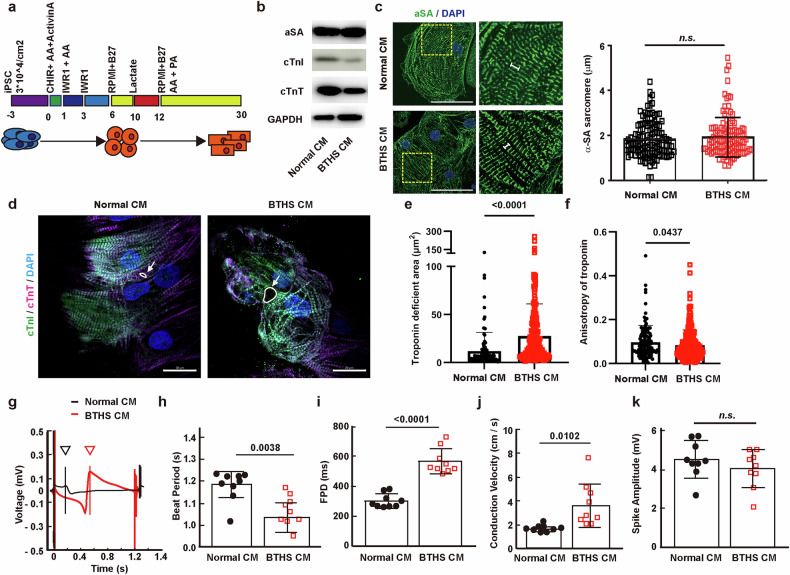
Barth syndrome (BTHS) is an ultrarare, infantile-onset, X-linked recessive mitochondrial disorder that primarily affects males, owing to mutations in TAFAZZIN, which catalyzes the remodeling of cardiolipin, a mitochondrial phospholipid required for oxidative phosphorylation. Mitochondrial transplantation is a novel technique to treat mitochondrial dysfunction by delivering healthy mitochondria to diseased cells or tissues. Here we explored the possibility of using stem-cell-derived cardiomyocytes as a source of mitochondrial transplantation to treat BTHS. We established induced pluripotent stem (iPS) cells from healthy individuals and from patients with BTHS and differentiated them into cardiomyocytes. The iPS-cell-differentiated cardiomyocytes (CMs) derived from patients with BTHS exhibited less expression of cardiomyocytes markers, such as α-SA, cTnT and cTnI, and smaller cell size than normal iPS-cell-derived CMs. Multielectrode array analysis revealed that BTHS CMs exhibited shorter beat period and longer field potential duration than normal CMs. In addition, mitochondrial morphology and function were impaired and mitophagy was decreased in BTHS CMs compared with normal CMs. Transplantation of mitochondria isolated from normal CMs induced mitophagy in BTHS CMs, mitigated mitochondrial dysfunction and promoted mitochondrial biogenesis. Furthermore, mitochondrial transplantation stimulated cardiac maturation and alleviated cardiac arrhythmia of BTHS CMs. These results suggest that normal CMs are useful for allogeneic transplantation in the treatment of mitochondrial diseases, including BTHS.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no conflicts of interest. Study approval: This study was approved by the IRB Boards of Pusan National University (#PNU IRB/2021_25_BR) and Pusan National University Yangsan Hospital (#L-2021-34).
Figures






Similar articles
-
Mitochondria-Homing Drug Mitochonic Acid 5 Improves Barth Syndrome Myopathy in a Human-Induced Pluripotent Stem Cell Model and Barth Syndrome Drosophila Model.FASEB J. 2025 Jun 30;39(12):e70739. doi: 10.1096/fj.202401856RRR. FASEB J. 2025. PMID: 40542649 Free PMC article.
-
Stem cell models of TAFAZZIN deficiency reveal novel tissue-specific pathologies in Barth syndrome.Hum Mol Genet. 2025 Jan 23;34(1):101-115. doi: 10.1093/hmg/ddae152. Hum Mol Genet. 2025. PMID: 39535077
-
Granulopoietic Dysregulation in a Patient-Tailored Mouse Model of Barth Syndrome.Stem Cell Rev Rep. 2025 Oct;21(7):2170-2187. doi: 10.1007/s12015-025-10945-1. Epub 2025 Aug 5. Stem Cell Rev Rep. 2025. PMID: 40762880 Free PMC article.
-
Metabolic impacts of long-chain fatty acids on cardiomyocyte maturation in neonatal mammalian hearts.Methods. 2025 Sep;241:114-127. doi: 10.1016/j.ymeth.2025.05.010. Epub 2025 May 29. Methods. 2025. PMID: 40449856 Review.
-
Nivolumab for adults with Hodgkin's lymphoma (a rapid review using the software RobotReviewer).Cochrane Database Syst Rev. 2018 Jul 12;7(7):CD012556. doi: 10.1002/14651858.CD012556.pub2. Cochrane Database Syst Rev. 2018. PMID: 30001476 Free PMC article.
Cited by
-
Mitochondrial dysfunction as a central hub linking Na+/Ca2+ homeostasis and inflammation in ischemic arrhythmias: therapeutic implications.Front Cardiovasc Med. 2025 Aug 12;12:1506501. doi: 10.3389/fcvm.2025.1506501. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40873621 Free PMC article. Review.
References
-
- Barth, P. G. et al. An X-linked mitochondrial disease affecting cardiac muscle, skeletal muscle and neutrophil leucocytes. J. Neurol. Sci.62, 327–355 (1983). - PubMed
-
- Neustein, H. B., Lurie, P. R., Dahms, B. & Takahashi, M. An X-linked recessive cardiomyopathy with abnormal mitochondria. Pediatrics64, 24–29 (1979). - PubMed
-
- Ferreira, C. et al. Barth Syndrome (eds M.P. Adam et al.) (University of Washington, 1993). - PubMed
-
- Jarvis, M., Garrett, P. & Svien, L. Gross motor development of a toddler with barth syndrome, an X-linked recessive disorder: a case report. Pediatr. Phys. Ther.13, 175–181 (2001). - PubMed
-
- Vanderniet, J. A., Benitez-Aguirre, P. Z., Broderick, C. R., Kelley, R. I. & Balasubramaniam, S. Barth syndrome with severe dilated cardiomyopathy and growth hormone resistance: a case report. J. Pediatr. Endocrinol. Metab.34, 951–955 (2021). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
