

AI-based large-scale screening of gastric cancer from noncontrast CT imaging
- PMID: 40555751
- PMCID: PMC12443630
- DOI: 10.1038/s41591-025-03785-6
AI-based large-scale screening of gastric cancer from noncontrast CT imaging
Abstract
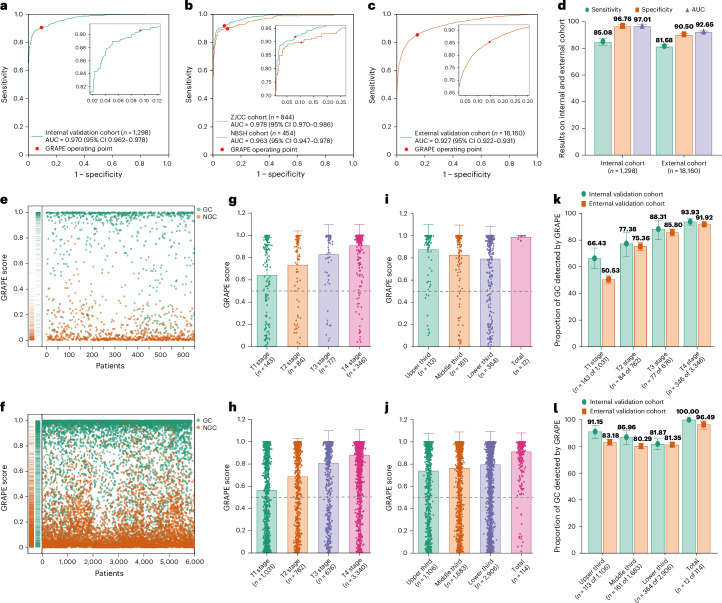
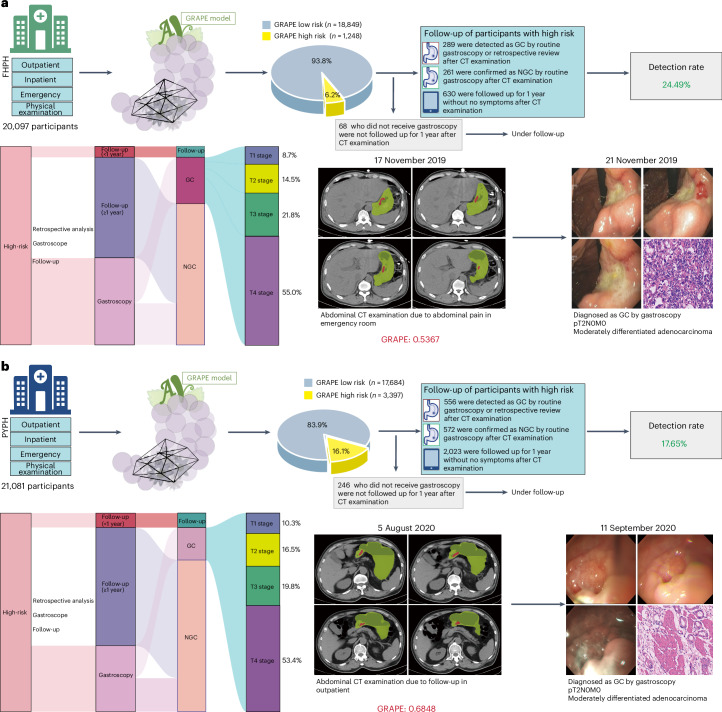
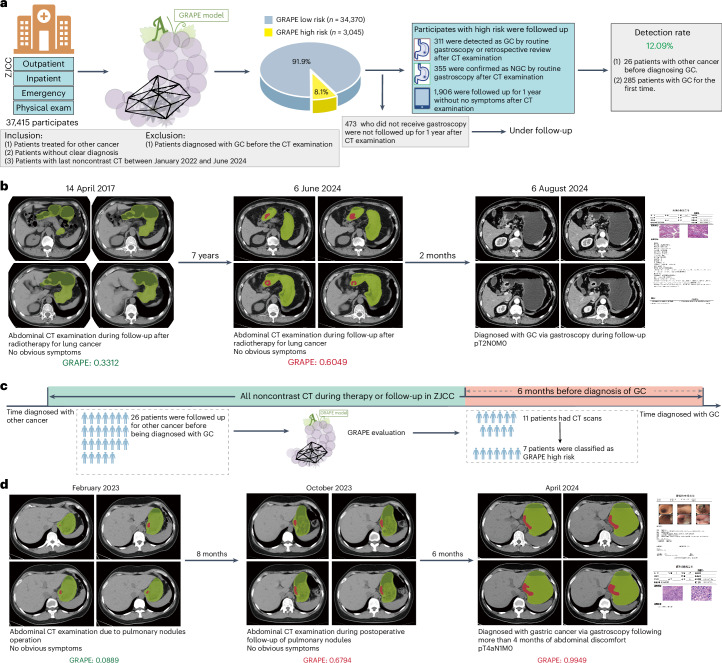
Early detection through screening is critical for reducing gastric cancer (GC) mortality. However, in most high-prevalence regions, large-scale screening remains challenging due to limited resources, low compliance and suboptimal detection rate of upper endoscopic screening. Therefore, there is an urgent need for more efficient screening protocols. Noncontrast computed tomography (CT), routinely performed for clinical purposes, presents a promising avenue for large-scale designed or opportunistic screening. Here we developed the Gastric Cancer Risk Assessment Procedure with Artificial Intelligence (GRAPE), leveraging noncontrast CT and deep learning to identify GC. Our study comprised three phases. First, we developed GRAPE using a cohort from 2 centers in China (3,470 GC and 3,250 non-GC cases) and validated its performance on an internal validation set (1,298 cases, area under curve = 0.970) and an independent external cohort from 16 centers (18,160 cases, area under curve = 0.927). Subgroup analysis showed that the detection rate of GRAPE increased with advancing T stage but was independent of tumor location. Next, we compared the interpretations of GRAPE with those of radiologists and assessed its potential in assisting diagnostic interpretation. Reader studies demonstrated that GRAPE significantly outperformed radiologists, improving sensitivity by 21.8% and specificity by 14.0%, particularly in early-stage GC. Finally, we evaluated GRAPE in real-world opportunistic screening using 78,593 consecutive noncontrast CT scans from a comprehensive cancer center and 2 independent regional hospitals. GRAPE identified persons at high risk with GC detection rates of 24.5% and 17.7% in 2 regional hospitals, with 23.2% and 26.8% of detected cases in T1/T2 stage. Additionally, GRAPE detected GC cases that radiologists had initially missed, enabling earlier diagnosis of GC during follow-up for other diseases. In conclusion, GRAPE demonstrates strong potential for large-scale GC screening, offering a feasible and effective approach for early detection. ClinicalTrials.gov registration: NCT06614179 .
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Alibaba Group has filed for patent protection ( CN116188392 ; the other application number is not currently in the public domain) for the work related to the methods of detection of GC in noncontrast CT. Y.X., Z.Z., Jianwei Xu, Z.Q., T.L., B.Y., J.Y., W.G., J.Z. and Ling Zhang are employees of Alibaba Group and own Alibaba stock as part of the standard compensation package. The other authors declare no competing interests.
Figures





References
-
- Smyth, E. C., Nilsson, M., Grabsch, H. I., van Grieken, N. C. & Lordick, F. Gastric cancer. Lancet396, 635–648 (2020). - PubMed
-
- Jiang, Y. et al. Predicting peritoneal recurrence and disease-free survival from CT images in gastric cancer with multitask deep learning: a retrospective study. Lancet Digit Health4, e340–e350 (2022). - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
