

Effect of Opioid-Free Versus Opioid Anesthesia on the Quality of Postoperative Recovery in Patients Receiving Laparoscopic Sleeve Gastrectomy
- PMID: 40555931
- PMCID: PMC12380946
- DOI: 10.1007/s11695-025-08008-y
Effect of Opioid-Free Versus Opioid Anesthesia on the Quality of Postoperative Recovery in Patients Receiving Laparoscopic Sleeve Gastrectomy
Abstract
Background: Opioids are commonly used in general anesthesia for pain management. However, they are related to obvious side effects. Patients with obesity undergoing laparoscopic sleeve gastrectomy are at higher risk of experiencing adverse effects associated with opioids. However, there is great heterogeneity in how to select and combine antinociceptive drugs to replace opioids. This randomized controlled double-blind study was conducted to evaluate the use effect of opioid-free anesthesia (OFA) in obese patients undergoing laparoscopic sleeve gastrectomy on the quality of postoperative recovery.
Methods: This prospective, parallel-group, double-blind, randomized controlled study included seventy-six patients undergoing laparoscopic sleeve gastrectomy in Beijing Friendship Hospital, Capital Medical University. Patients were randomly assigned to OFA group or opioid-based anesthesia (OBA) group. The primary outcome included the 15-item recovery quality scale (QOR-15). Secondary measures included intraoperative hemodynamic stability, intraoperative operation information, duration of until postoperative PACU Aldrete score > 9 points, anesthesia-related complication, and number of analgesic pump presses.
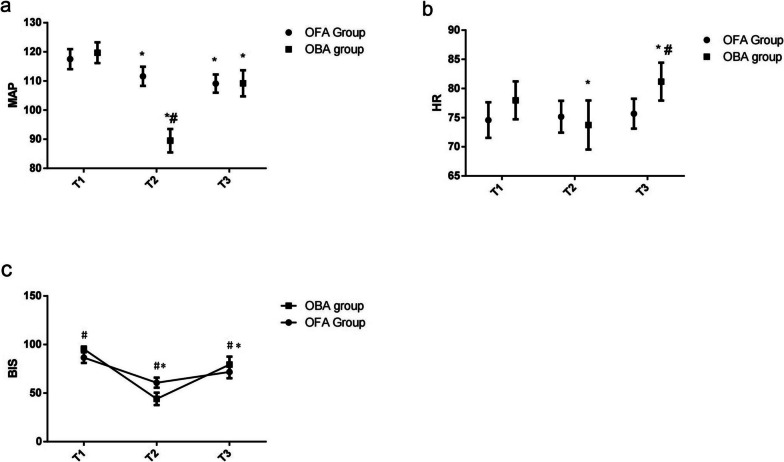
Results: The scores of QOR-15 in OFA group were higher than that in OBA group at 24 h and 48 h after surgery. The total dose of propofol required in OFA group was statistically less than that in OBA group. Patients in the OBA group had significantly lower bispectral index (BIS) values and lower levels of MAP at T2 (after intubation) than those in the OFA group patients in the OBA group. Patients in the OFA group showed significantly lower levels of heart rate (HR) at T3 (after abdominal closure) when compared to the OBA group. The changing trend of visual analog scale (VAS) and OBAS scores recorded after surgery were similar between both groups and the VAS and Overall Benefit of Analgesia Scale (OBAS) scores in OBA group were obviously higher than those in OFA group in each time point. The Rhodes Index of Nausea and Vomiting in OBA group were obviously higher than those in OFA group in each time point.
Conclusions: OFA significantly improved postoperative recovery quality as evidenced by higher QOR-15 scores, reduced postoperative nausea and vomiting (PONV), lower pain scores and decreased opioid requirements compared to OBA. Although duration of awakening from anesthesia was prolonged, OFA demonstrated superior recovery outcomes and fewer complications supporting its clinical utility in obese patients undergoing laparoscopic sleeve gastrectomy.
Keywords: Laparoscopic sleeve gastrectomy; Obesity; Opioid-based anesthesia; Opioid-free anesthesia; Postoperative recovery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Consent for Publication: Not applicable. Competing interest: The authors declare no competing interests.
Figures


Similar articles
-
Opioid-Free Anesthesia Improved the Quality of Recovery After Thyroidectomy Through Pre-Emptive and Preventive Analgesia: A Randomized Controlled Trial.Drug Des Devel Ther. 2025 Jun 19;19:5243-5254. doi: 10.2147/DDDT.S520856. eCollection 2025. Drug Des Devel Ther. 2025. PMID: 40552090 Free PMC article. Clinical Trial.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Opioid-free anaesthesia protocol based on thoracic paravertebral block enhances postoperative recovery after breast cancer surgery: A two-center, prospective, randomized, controlled trial.J Clin Anesth. 2025 Jul;105:111904. doi: 10.1016/j.jclinane.2025.111904. Epub 2025 Jun 17. J Clin Anesth. 2025. PMID: 40532358 Clinical Trial.
-
Surgery for weight loss in adults.Cochrane Database Syst Rev. 2014 Aug 8;2014(8):CD003641. doi: 10.1002/14651858.CD003641.pub4. Cochrane Database Syst Rev. 2014. PMID: 25105982 Free PMC article.
-
Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults.Cochrane Database Syst Rev. 2018 Jun 4;6(6):CD009642. doi: 10.1002/14651858.CD009642.pub3. Cochrane Database Syst Rev. 2018. PMID: 29864216 Free PMC article.
References
-
- Batchelder AJ, Williams R, Sutton C, et al. The evolution of minimally invasive bariatric surgery [J]. J Surg Res. 2013;183(2):559–66. - PubMed
-
- Wang Y, Wang L, Qu W. New national data show alarming increase in obesity and noncommunicable chronic diseases in China. Eur J Clin Nutr. 2017;71(1):149–50. - PubMed
-
- Engin AB, Engin A. Adiponectin-resistance in obesity Obes Lipotoxicity. 2017;960:415–41. - PubMed
-
- Ming X, Yang M, Chen X. Metabolic bariatric surgery as a treatment for obstructive sleep apnea hypopnea syndrome: review of the literature and potential mechanisms. Surg Obes Relat Dis. 2021;17:215–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
