

Magnitude, outcome, and predictors of mortality in perforated peptic ulcer disease: a retrospective study in Jigjiga town, Ethiopia
- PMID: 40556000
- PMCID: PMC12186399
- DOI: 10.1186/s13017-025-00628-0
Magnitude, outcome, and predictors of mortality in perforated peptic ulcer disease: a retrospective study in Jigjiga town, Ethiopia
Abstract
Background: Peptic ulcer perforation (PUP) is a surgical emergency and life-threatening complication affecting 2-10% of peptic ulcer disease (PUD) patients. Delayed diagnosis and surgical management are associated with significant morbidity and mortality. This study assessed the magnitude and outcome of PUP among patients operated on at two public hospitals in Jigjig town, Ethiopia.
Methods: A 3-year hospital-based retrospective cross-sectional study was conducted on 130 patients operated for PUP at the study hospitals in Jigjig from April 1st, 2018, to July 30th, 2021. Data were collected from medical records. Bivariate analysis identified key factors impacting outcomes in PUP patients.
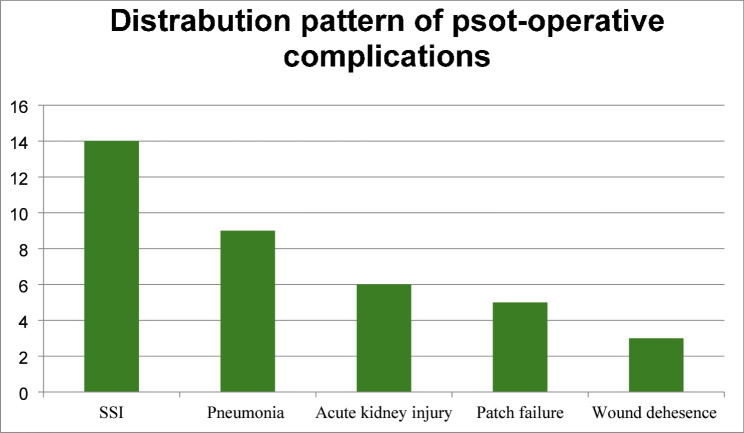
Results: The cohort had a male-to-female ratio of 8.7:1, and a mean age of 38 ± 13.3 years, with 48.8% smokers and 56.6% chat chewers. Duodenal perforations accounted for 93.7% of cases, with post-operative complications in 29.1% and an in-hospital mortality rate of 5.5%. Significant predictors of morbidity and mortality included advanced age (AOR 23.88), comorbidities (AOR 26.80), pre-operative hypotension (AOR 32.33), and delayed hospital presentation (AOR 30.10).
Conclusions: Male predominance, younger age, high smoking and chat chewing rates, and primarily duodenal perforations are common in perforated peptic ulcer cases. Advanced age, comorbidities, pre-operative hypotension, and delayed hospital presentation significantly increase postoperative complications and mortality, emphasizing the need for timely intervention and targeted public health measures to improve patient outcomes. Early intervention and careful management of comorbidities are crucial to improve survival and reduce complications in patients with PUP.
Keywords: Jigjiga and Ethiopia; Outcome; Perforated peptic ulcer disease.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted following the ethical standards of Jigjiga University, Ethiopia, and the necessary documents were acquired. Consent to participate: All participants were informed about the study’s purpose and procedures and gave their voluntary consent to participate. They were assured of the confidentiality of their responses and informed of their right to withdraw at any time without consequence. Consent for publication: All participants were informed that the results of the study will be published in an academic or public format. They provided their consent for the use of anonymized data in publications, with assurance that their identities would not be disclosed. Competing interests: The authors declare no competing interests.
Figures


References
-
- Bertleff MJOE, Lange JF. Perforated peptic ulcer disease: a review of history and treatment., Dig. Surg., 2010;27(3):161–169, 10.1159/000264653 - PubMed
-
- Ugochukwu AI, Amu OC, Nzegwu MA, Dilibe UC. Acute perforated peptic ulcer: on clinical experience in an urban tertiary hospital in Southeast Nigeria. Int J Surg. 2013;11(3):223–7. 10.1016/j.ijsu.2013.01.015 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
