

Syringomyelia Associated with Magendie's Foramen Obstruction Due to Probably Congenital Gliomesenchymal Anomaly
- PMID: 40556636
- PMCID: PMC12187467
- DOI: 10.2176/jns-nmc.2025-0041
Syringomyelia Associated with Magendie's Foramen Obstruction Due to Probably Congenital Gliomesenchymal Anomaly
Abstract
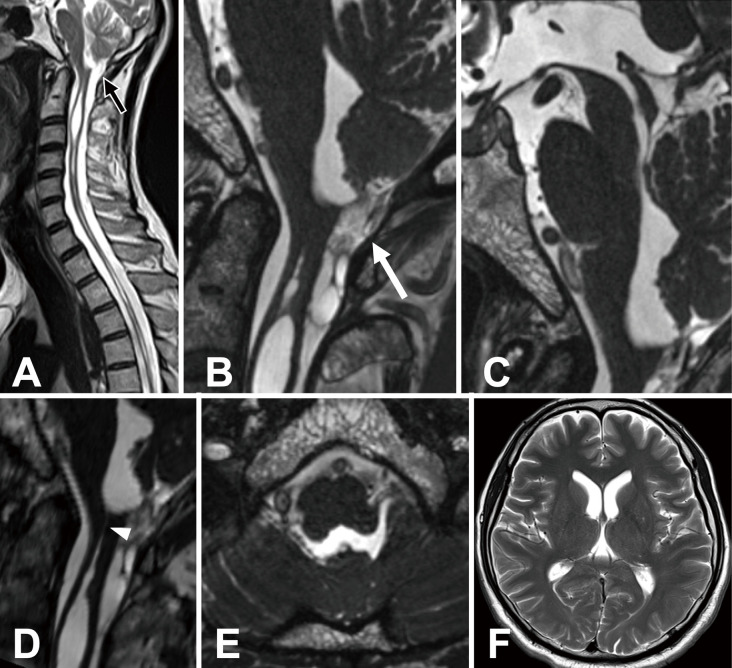
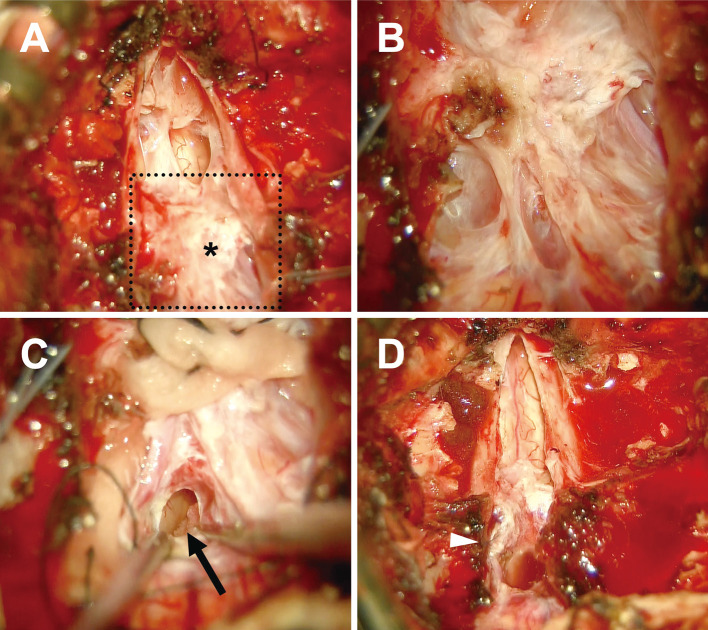
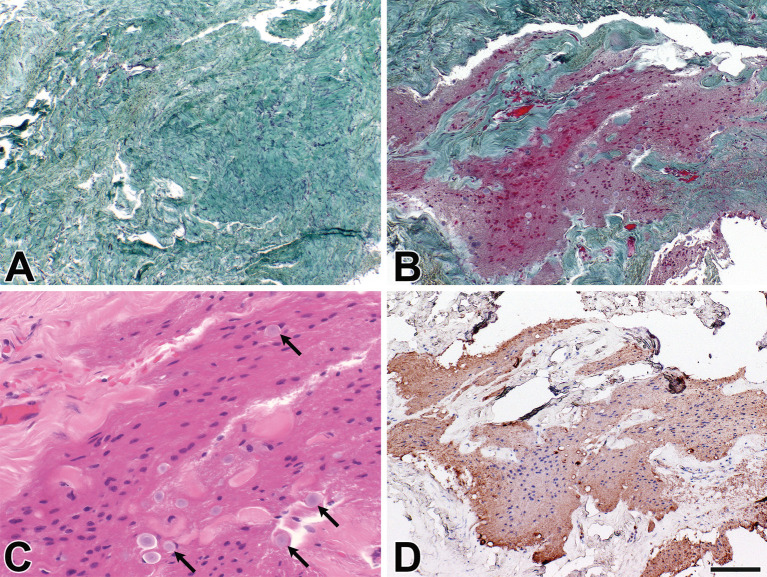
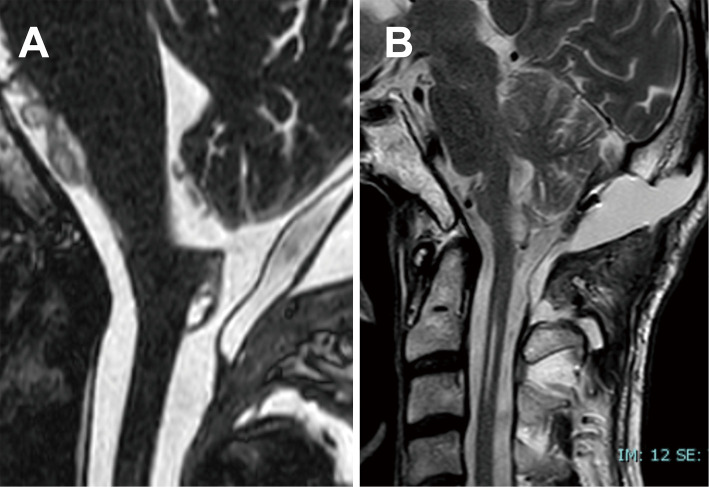
We report a case of syringomyelia in a 55-year-old man with a unique obstruction of Magendie's foramen. Spinal magnetic resonance imaging revealed a large syrinx extending from C1 to C3, with intermittent syringomyelia extending down to Th11. While the obstruction was not clearly evident on T2-weighted imaging, three-dimensional constructive interference in steady-state imaging demonstrated a thickened membranous tissue blocking the cerebrospinal fluid outlet, leading to syrinx formation. Surgical intervention, involving the resection of the thickened membrane to open the foramen of Magendie, resulted in considerable improvement in the syringomyelia and neurological symptoms. Histopathological examination revealed gliomesenchymal tissue, suggesting an embryonic origin of the obstruction. This case highlights the importance of detailed imaging, particularly three-dimensional constructive interference in steady-state sequence, in diagnosing foramen of Magendie obstruction and the potential for successful surgical treatment in selected cases. Histopathological examination is crucial for differentiating gliomesenchymal tissue from adhesive arachnoiditis.
Keywords: 3D-CISS; Magendie's foramen; gliomesenchymal tissue; membranous obstruction; syringomyelia.
© 2025 The Japan Neurosurgical Society.
Conflict of interest statement
All authors have no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous