

Follicular dendritic cell sarcoma: a great mimicker with unpredictable clinical course-experience from a tertiary care cancer center in India
- PMID: 40556670
- PMCID: PMC12185445
- DOI: 10.3389/fonc.2025.1544803
Follicular dendritic cell sarcoma: a great mimicker with unpredictable clinical course-experience from a tertiary care cancer center in India
Abstract
Background: Follicular dendritic cell sarcoma (FDCS) is a rare mesenchymal malignant tumor derived from follicular dendritic cells. FDCS arises mainly from lymph nodes and rarely are extranodal. Diagnostic dilemma occurs due to the same micromorphology as other sarcomas and lymphomas. Curative radical resection is the standard therapy, and adjuvant treatment is not defined. For unresectable disease, chemotherapy and radiotherapy are indicated with variable response rates. Due to its rarity, a standard treatment is not yet defined.
Objective: This study aims to analyze the clinicopathological features, treatment patterns, and survival outcome of FDCS cases in our institution.
Methodology: The study was conducted in the Department of Medical Oncology State Cancer Institute, Sher I Kashmir Institute of Medical Sciences (SKIMS), Srinagar, Jammu and Kashmir, India. Biopsy-proven FDCS patients were identified through the hospital-based registry from January 1, 2020 to December 31, 2023.
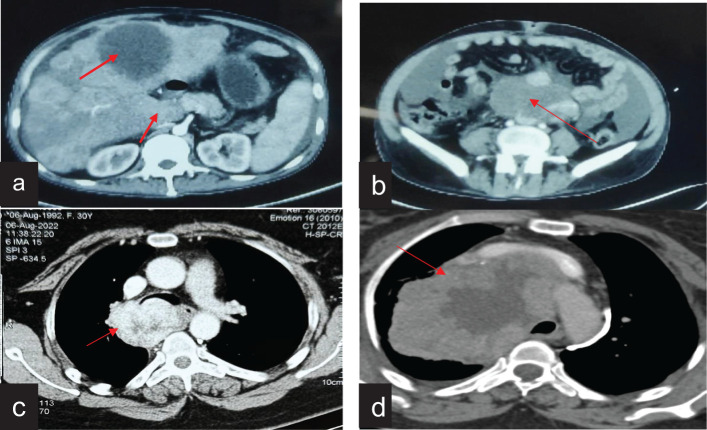
Results: A total of six patients were diagnosed during the study period. The median age was 28 years (range, 21-51 years). There were four male and two female patients, with male-to-female ratio of 2:1. Common symptoms were abdominal pain (50%) and cough and dyspnea (33.3%). Four patients (66.6%) had nodal involvement with retroperitoneum and mediastinum in two cases each. Three patients had extranodal involvement, with the colon in two and with the liver in one. Five patients were initially misdiagnosed as non-Hodgkin's lymphoma, soft tissue sarcoma, neurogenic tumor, and carcinoma. The treatments offered were surgery, chemotherapy, targeted therapy, radiotherapy, and observation. Four patients were alive at a median follow-up of 12 months, with three patients having no evidence of disease and one case living with the disease. Two patients had succumbed to the disease.
Conclusion: The study described the clinicopathological characteristics, diagnostic challenges, and management difficulties in FDCS patients. Due to the rarity of this disease, high expertise is needed to diagnose FDCS; otherwise, the diagnosis usually gets delayed.
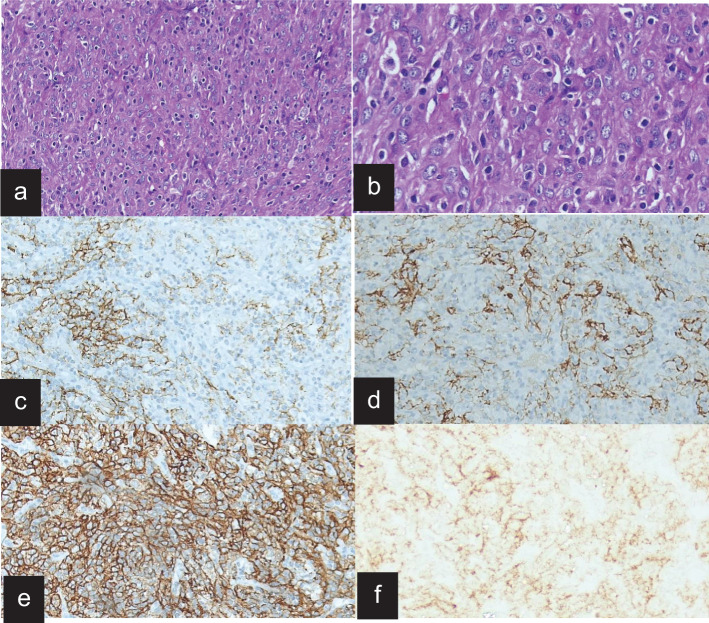
Keywords: dendritic cells; follicular dendritic cell sarcoma; histopathology; immunohistochemistry; mimicker.
Copyright © 2025 Ibrahim, Mir, Bagdadi, Sofi, Khanday, Wani, Regmi, Bhat, Syed, Guru, Wani and Qadri.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Nivolumab for adults with Hodgkin's lymphoma (a rapid review using the software RobotReviewer).Cochrane Database Syst Rev. 2018 Jul 12;7(7):CD012556. doi: 10.1002/14651858.CD012556.pub2. Cochrane Database Syst Rev. 2018. PMID: 30001476 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Enhanced CT Findings in a Case of Recurrent Pelvic Follicular Dendritic Cell Sarcoma.Curr Med Imaging. 2024;20:e15734056273583. doi: 10.2174/0115734056273583231210055038. Curr Med Imaging. 2024. PMID: 38389367
References
LinkOut - more resources
Full Text Sources