

Bone Graft Expansion in Cranioplasty Using a Split-Bone Technique
- PMID: 40556979
- PMCID: PMC12187105
- DOI: 10.7759/cureus.84790
Bone Graft Expansion in Cranioplasty Using a Split-Bone Technique
Abstract
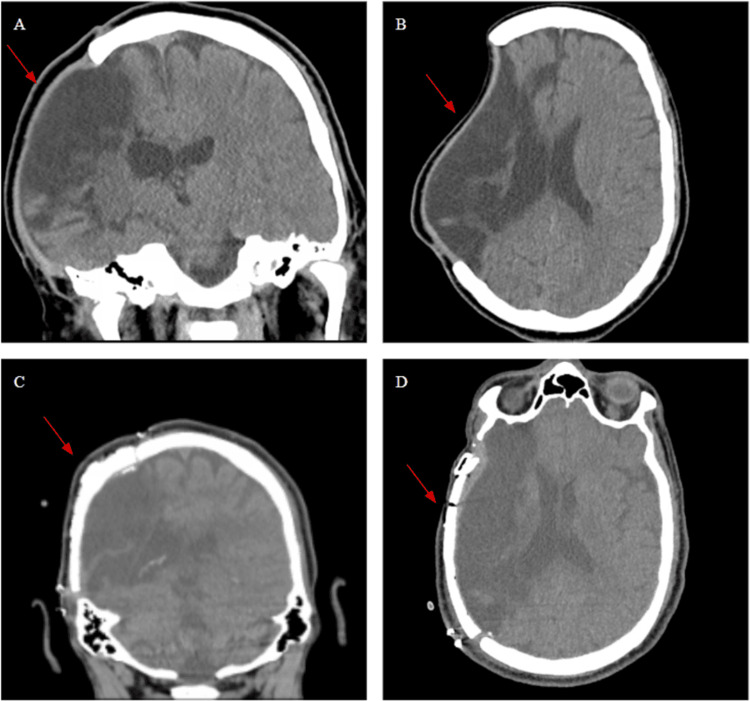
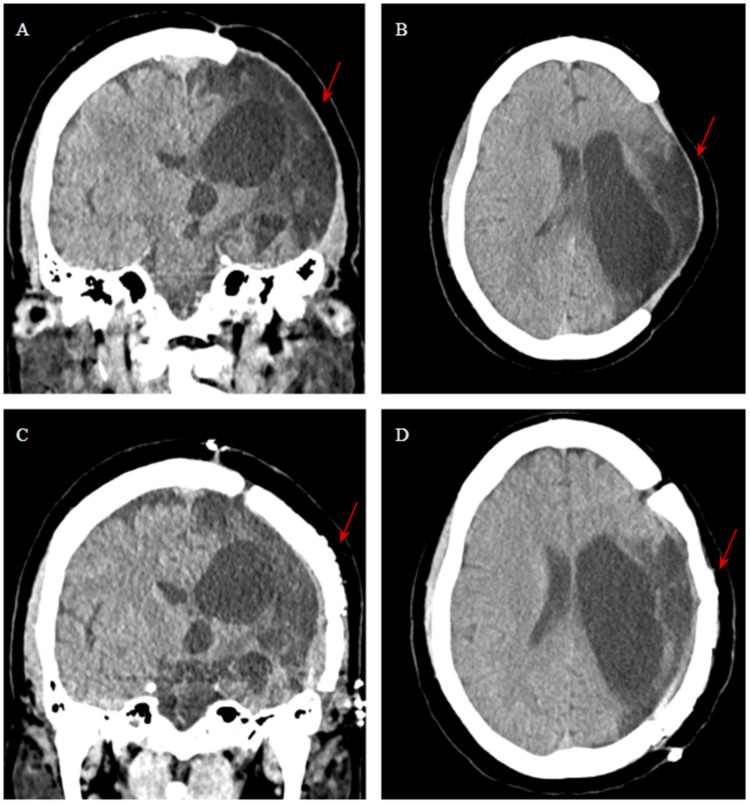
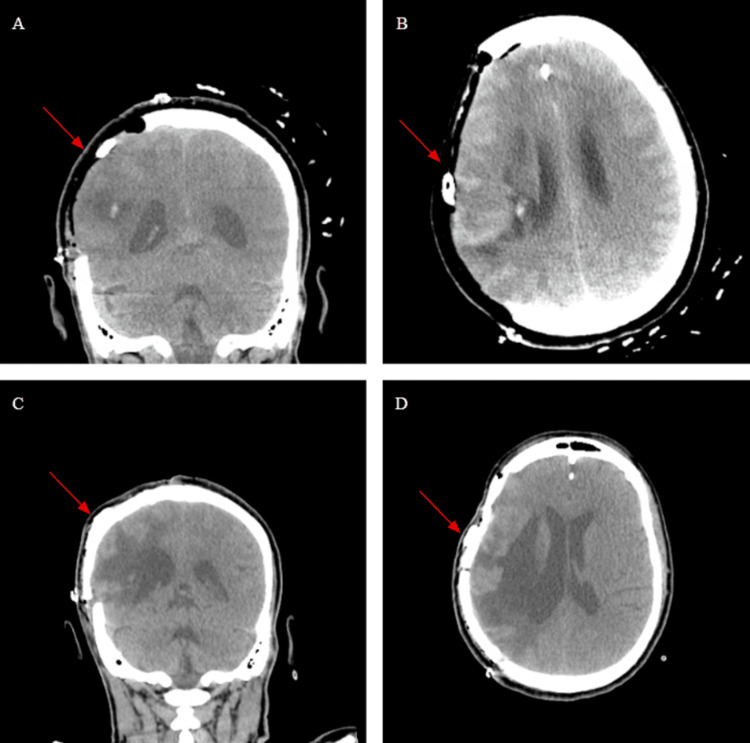
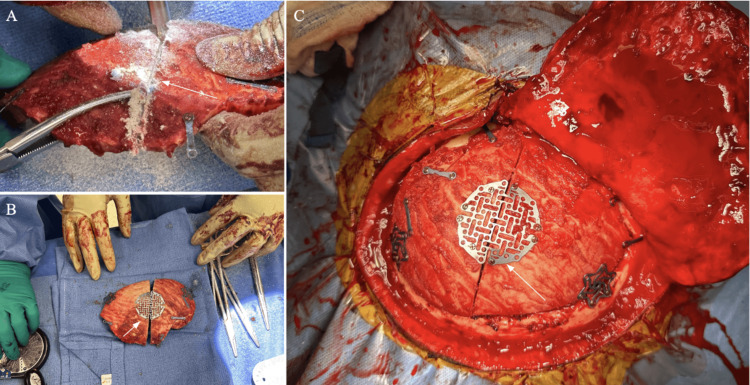
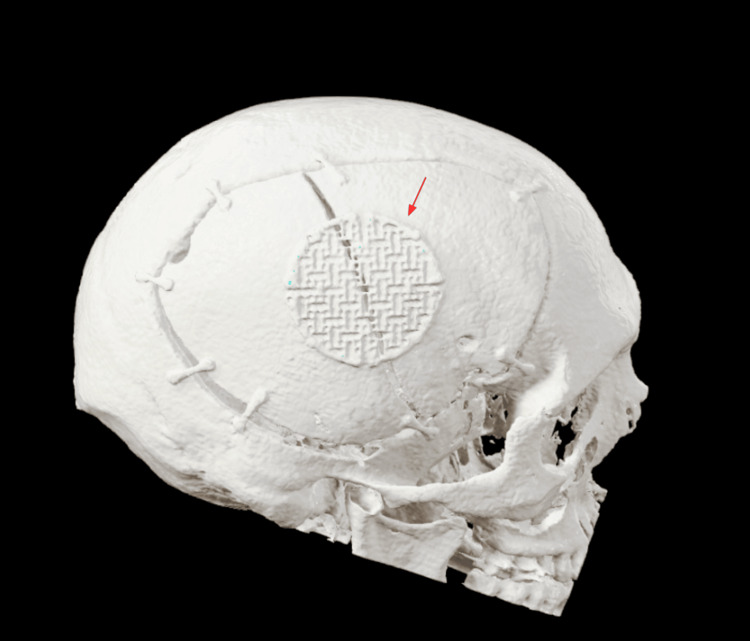
Decompressive hemicraniectomy (DHC) is performed in emergent cases of uncontrollable intracranial hypertension in which noninvasive procedures or medications are not able to safely maintain pressure within the cranium, increasing the risk of morbidity and mortality. The native bone flap is then replaced, a procedure referred to as cranioplasty, nearly three to six months after injury to allow time for brain relaxation. However, in cases with persistent cerebral edema at the time of cranioplasty, techniques are often applied intraoperatively, including mannitol, external ventricular drain, or lumbar drain placement. To avoid the risks of delaying the procedure or drain placement, we demonstrate a novel technique of splitting the bone flap to adequately increase the size and flexibility. Three patients with a mean age of 44 underwent this novel technique during cranioplasty due to persistent brain edema following a DHC. The new operative technique was successfully performed to compensate for the lingering edema, and all three patients were monitored postoperatively, showing no complications. In this study we demonstrate a new technique to alter bone flap size and flexibility during cranioplasty cases with persistent brain edema, avoiding the need for invasive drain placement. All patients experienced no complications or new cranial/skull defects postoperatively.
Keywords: cerebral edema; craniectomy; cranioplasty; craniotomy; neurocritical care.
Copyright © 2025, Talbot et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Fornix-based versus limbal-based conjunctival trabeculectomy flaps for glaucoma.Cochrane Database Syst Rev. 2021 Aug 26;8(8):CD009380. doi: 10.1002/14651858.CD009380.pub3. Cochrane Database Syst Rev. 2021. PMID: 34437715 Free PMC article.
-
Heliox for croup in children.Cochrane Database Syst Rev. 2021 Aug 16;8(8):CD006822. doi: 10.1002/14651858.CD006822.pub6. Cochrane Database Syst Rev. 2021. PMID: 34397099 Free PMC article.
-
A systematic review and meta-analysis of factors involved in bone flap resorption after decompressive craniectomy.Neurosurg Rev. 2022 Jun;45(3):1915-1922. doi: 10.1007/s10143-022-01737-z. Epub 2022 Jan 21. Neurosurg Rev. 2022. PMID: 35061139
-
Exercise versus airway clearance techniques for people with cystic fibrosis.Cochrane Database Syst Rev. 2022 Jun 22;6(6):CD013285. doi: 10.1002/14651858.CD013285.pub2. Cochrane Database Syst Rev. 2022. PMID: 35731672 Free PMC article.
References
-
- Decompressive craniectomy. Schirmer CM, Ackil AA Jr, Malek AM. Neurocrit Care. 2008;8:456–470. - PubMed
-
- Malignant middle cerebral artery infarction: clinical characteristics, treatment strategies, and future perspectives. Huttner HB, Schwab S. Lancet Neurol. 2009;8:949–958. - PubMed
-
- Pinto VL, Tadi P, Adeyinka A. StatPearls. Vol. 13. StatPearls Publishing; 2024. Increased intracranial pressure. - PubMed
-
- Decompressive craniectomy and traumatic brain injury: a review. Alvis-Miranda H, Castellar-Leones SM, Moscote-Salazar LR. https://pubmed.ncbi.nlm.nih.gov/27162826/ Bull Emerg Trauma. 2013;1:60–68. - PMC - PubMed
-
- Refractory intracranial hypertension: the role of decompressive craniectomy. Smith M. Anesth Analg. 2017;125:1999–2008. - PubMed
Publication types
LinkOut - more resources
Full Text Sources