

Unilateral Hearing Loss as the Sole Presentation of Extensive Intracranial Epidermoid Cyst: A Case Report
- PMID: 40556983
- PMCID: PMC12186845
- DOI: 10.7759/cureus.84721
Unilateral Hearing Loss as the Sole Presentation of Extensive Intracranial Epidermoid Cyst: A Case Report
Abstract
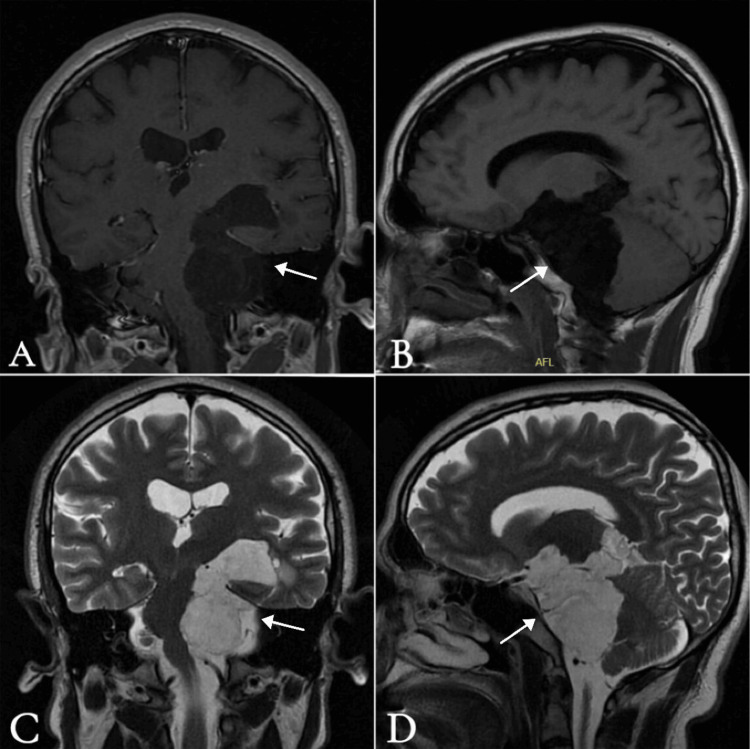
Epidermoid cysts are rare congenital tumors of the central nervous system. These histologically benign, slow-growing lesions form when ectodermal cells become trapped during the closure of the neural tube. Histologically, they consist of a core composed of keratin, desquamated epithelial cells, and cholesterol, surrounded by a layer of stratified squamous epithelium. Clinical features depend on the lesion's location. In the cerebellopontine angle (CPA), they typically present with tinnitus, vertigo, hearing loss, and facial weakness, with or without cerebellar signs and symptoms. Unilateral hearing loss as the sole presenting symptom is uncommon in the setting of a large, extensive cyst and may delay diagnosis. A 35-year-old male presented with progressive left-sided hearing loss for one year, without vertigo, tinnitus, or other neurological symptoms. Audiological testing revealed severe-to-profound sensorineural hearing loss in the left ear. Temporal bone computed tomography and brain magnetic resonance imaging showed a large, extra-axial cystic lesion in the left CPA with characteristic diffusion-weighted imaging restriction, consistent with an epidermoid cyst. The lesion caused significant mass effect, including compression of the brainstem, cranial nerves, basilar artery, left vertebral artery, and left posterior cerebral artery. The patient underwent successful surgical excision via a retrosigmoid suboccipital craniotomy. Histopathological examination confirmed the diagnosis of an epidermoid cyst. This case report highlights an unusual presentation of an extensive epidermoid cyst in the left CPA that manifested solely as unilateral hearing loss, underscoring the diagnostic challenges posed by this rare lesion. The findings emphasize the importance of considering atypical presentations of intracranial tumors in the differential diagnosis of patients with unexplained hearing loss.
Keywords: cerebellopontine angle; cranial nerve compression; craniotomy; epidermoid cyst; hearing loss; inclusion cyst; intracranial tumor.
Copyright © 2025, Alosaimi et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Epidermoid cysts of the cerebellopontine angle: clinical features and treatment outcomes. Czernicki T, Kunert P, Nowak A, Wojciechowski J, Marchel A. Neurol Neurochir Pol. 2016;50:75–82. - PubMed
-
- Clinical characteristics and diagnostic imaging of epidermoid tumors. Nagasawa D, Yew A, Safaee M, Fong B, Gopen Q, Parsa AT, Yang I. J Clin Neurosci. 2011;18:1158–1162. - PubMed
-
- Cerebellopontine angle epidermoid cyst presenting with only trigeminal neuralgia: a retrospective study at the single-center in Vietnam. Do PT, Nguyen CK, Le VT. Interdisc Neurosurg. 2024;37:101987.
-
- Zito PM, Scharf R. StatPearls [Internet] Treasure Island: StatPearls Publishing; [ Nov; 2025 ]. 2025 Jan-. Epidermoid cyst. - PubMed
Publication types
LinkOut - more resources
Full Text Sources