

Mammography screening and incidence of ductal carcinoma in situ of the breast in Italy: an age-period-cohort analysis
- PMID: 40557614
- PMCID: PMC12188216
- DOI: 10.1093/ije/dyaf102
Mammography screening and incidence of ductal carcinoma in situ of the breast in Italy: an age-period-cohort analysis
Abstract
Background: The increasing incidence of ductal carcinoma in situ (DCIS) of the breast is attributed to mammography screening, but the trend has so far been evaluated only descriptively.
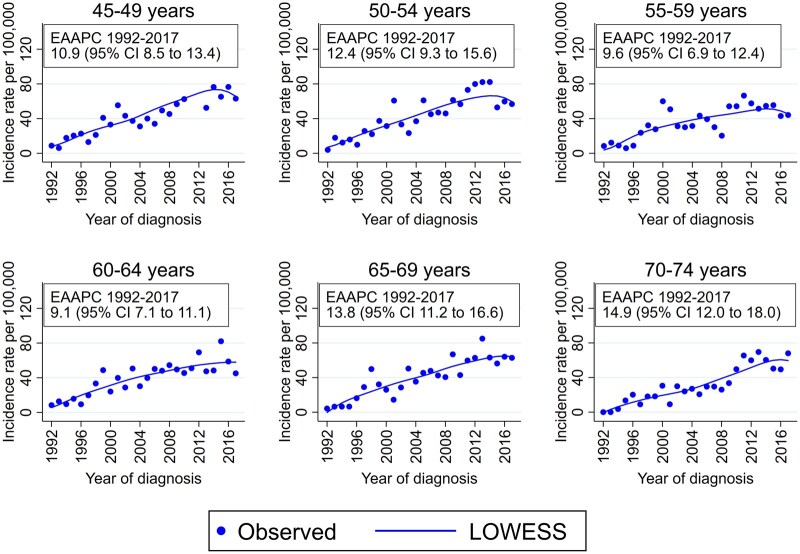
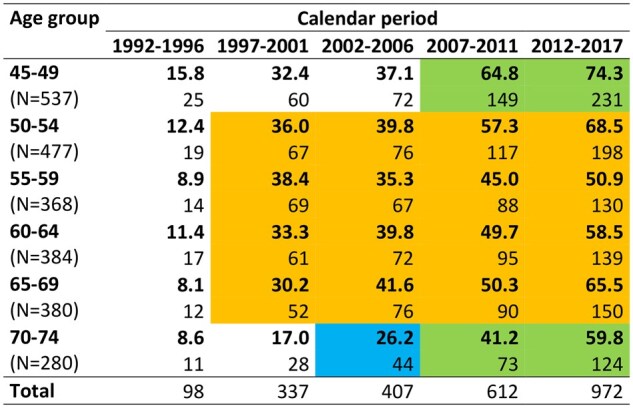
Methods: We report an age-period-cohort modelling analysis of the incidence trend (1992-2017) observed among screening-aged women living in a region of northern Italy, where a mammography screening programme was implemented in 1996-98 (age 50-69 years) and 2010-14 (age 45-49 and 70-74 years).
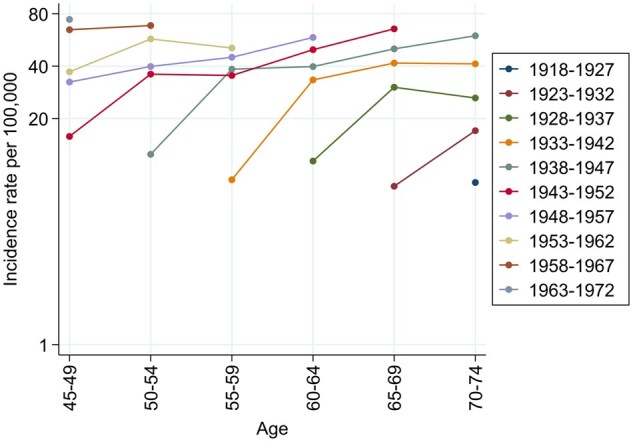
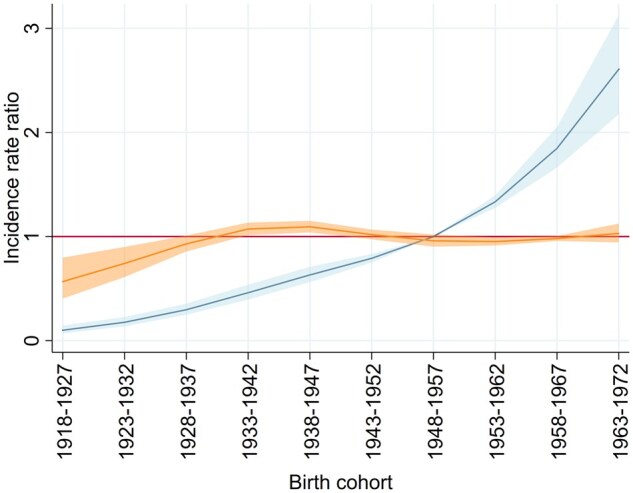
Results: The incidence of DCIS increased by an annual average of 9.1% (age 60-64 years) to 14.9% (age 70-74 years). The incidence peak followed a complex age-time pattern indicating an interaction between age and period, which suggested a cohort effect explained by the screening programme. In the age-period-cohort analysis, the birth cohort had a 2-fold effect. The nonlinear effect consisted of an increase in incidence for the generations of 1933-42 and 1943-52, targeted by screening since 1997, and of a second increase for the cohort of 1963-72, first invited in 2010. Taking into account the early excess incidence due to the introduction of the screening programme, the linear effect consisted of an annual 4.0% increase in the risk of DCIS for all successive birth cohorts or calendar periods, which was only partially attributable to the programme.
Conclusions: The increase in incidence rates resulted from an increased detection of DCIS through the screening programme and from an uptrend in the risk of diagnosis that can be attributed either to long-term changes in diagnostic scrutiny independent of the programme or to an increased exposure to risk factors.
Keywords: age-period-cohort analysis; breast neoplasms; ductal carcinoma in situ; incidence; mammography; mass screening.
© The Author(s) 2025. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures

Similar articles
-
Retrospective quantification of background incidence and stage distribution of breast cancer for the mammography screening pilot project in Wiesbaden, Germany.J Cancer Res Clin Oncol. 2008 Jan;134(1):29-35. doi: 10.1007/s00432-007-0239-4. Epub 2007 Jun 30. J Cancer Res Clin Oncol. 2008. PMID: 17602243 Free PMC article.
-
Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes.J Natl Cancer Inst. 2010 Feb 3;102(3):170-8. doi: 10.1093/jnci/djp482. Epub 2010 Jan 13. J Natl Cancer Inst. 2010. PMID: 20071685
-
Imaging findings for response evaluation of ductal carcinoma in situ in breast cancer patients treated with neoadjuvant systemic therapy: a systematic review and meta-analysis.Eur Radiol. 2023 Aug;33(8):5423-5435. doi: 10.1007/s00330-023-09547-7. Epub 2023 Apr 5. Eur Radiol. 2023. PMID: 37020070 Free PMC article.
-
Interventions targeted at women to encourage the uptake of cervical screening.Cochrane Database Syst Rev. 2021 Sep 6;9(9):CD002834. doi: 10.1002/14651858.CD002834.pub3. Cochrane Database Syst Rev. 2021. PMID: 34694000 Free PMC article.
-
Mammography in combination with breast ultrasonography versus mammography for breast cancer screening in women at average risk.Cochrane Database Syst Rev. 2023 Mar 31;3(3):CD009632. doi: 10.1002/14651858.CD009632.pub3. Cochrane Database Syst Rev. 2023. PMID: 36999589 Free PMC article.
References
-
- Virnig BA, Tuttle TM, Shamliyan T, Kane RL. Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. J Natl Cancer Inst 2010;102:170–8. - PubMed
-
- Jacklyn G, Morrell S, McGeechan K et al. Carcinoma in situ of the breast in New South Wales, Australia: current status and trends over the last 40 year. Breast 2018;37:170–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
