

The Value of Thin Layer Cytology in Cancer Patients' Pericardial Effusions
- PMID: 40558249
- PMCID: PMC12192277
- DOI: 10.3390/curroncol32060306
The Value of Thin Layer Cytology in Cancer Patients' Pericardial Effusions
Abstract
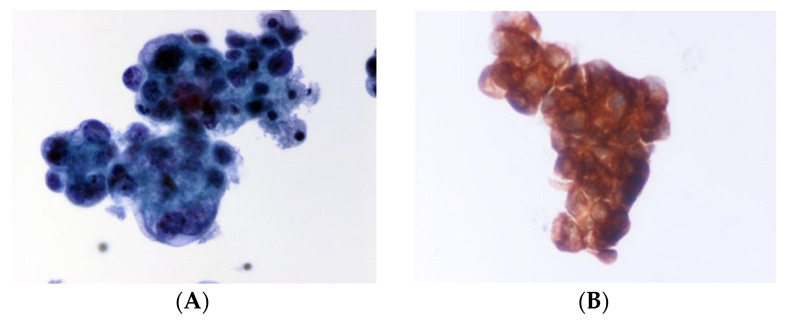
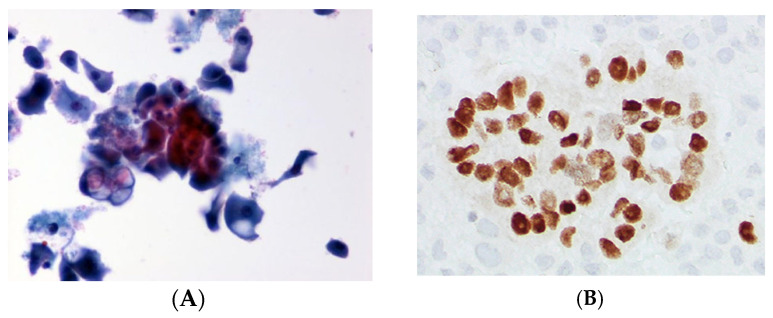
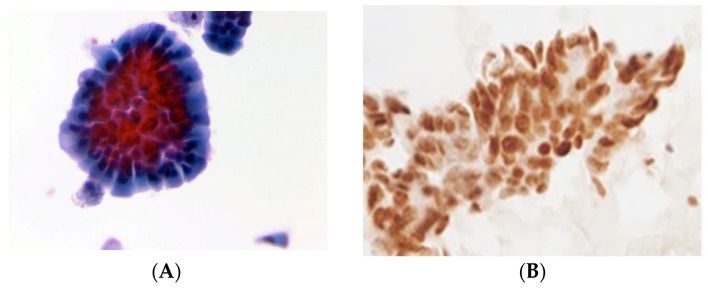
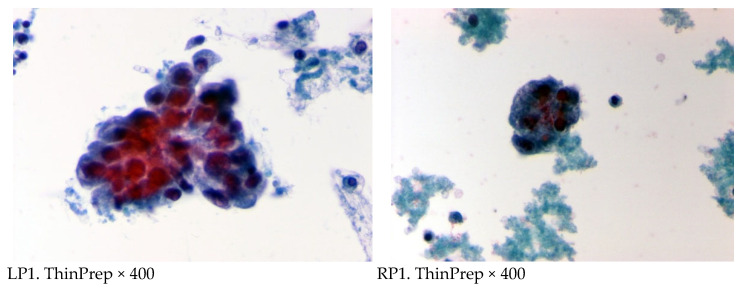
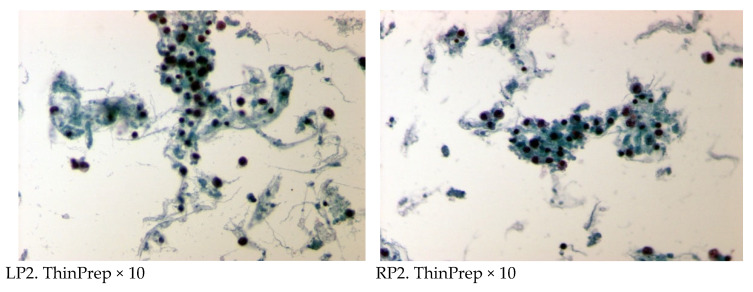
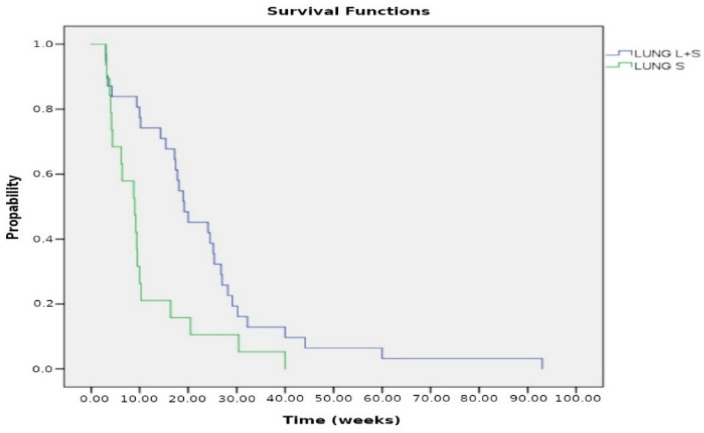
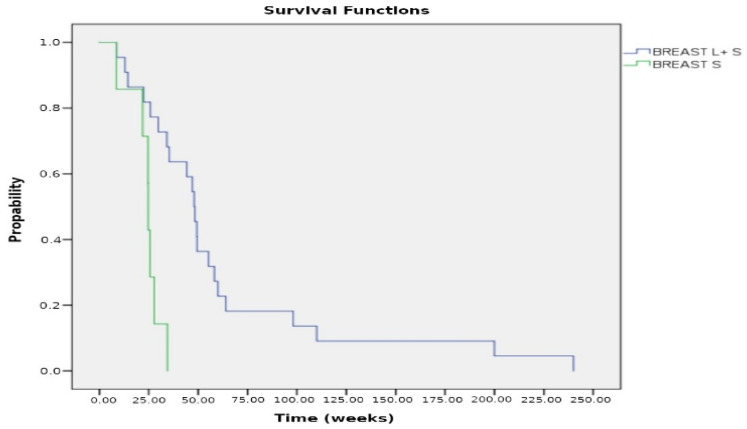
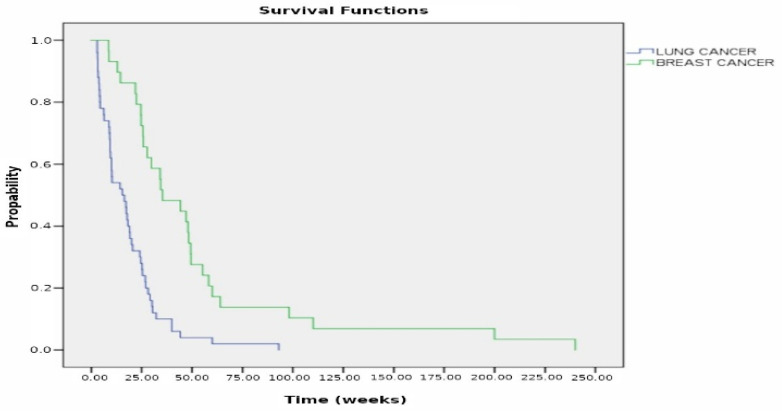
Objective: Early diagnosis and treatment of metastatic pericardial disease are crucial to prevent the life-threatening complication of cardiac tamponade. Thin Layer Cytology (TLC), a widely adopted technique in cytology, has gained significant acceptance for most specimens. Our study aimed to assess the utility of TLC in diagnosing metastatic neoplasms and their origins in pericardial effusions, as well as monitoring response to chemotherapy. Methods: We examined 184 pericardial fluids collected by pericardiocentesis and processed using the ThinPrep liquid-based technique. Various immunocytochemical markers were used to determine the site of metastatic neoplasms. We also evaluated the response to therapy in 53 patients with lung and breast cancer. Results: Out of 184 specimens, 113 pericardial fluids were diagnosed as positive for malignancy, while 71 were negative. Twenty-three cases of unknown primary site were included in the total positive cases. Ninety cases positive for malignancy had a known primary site of origin, including 31 lung carcinomas, 22 breast carcinomas, 10 ovarian carcinomas, 6 T-cell lymphomas, 3 urinary bladder carcinomas, 4 renal carcinomas, 5 adenocarcinomas of the colon, 5 prostate carcinomas, 2 parotid adenocarcinomas, and 2 melanomas. Regarding the 53 cases with chemotherapy treatment, the cytologic examination of pericardial fluid showed a remarkable reduction in neoplastic burden after the third dose of cisplatin or thiotepa instilled into the pericardial cavity. ThinPrep provided excellent preservation of cytomorphological features, high cellularity per slide, and a clear background. This comprehensive analysis provides crucial information about the types and distribution of cancerous cells present in the samples. Conclusions: Thin Layer Cytology (TLC) is a valuable diagnostic tool for detecting metastatic pericardial malignancy. It allows the examination of exfoliated cells from the pericardial fluid, providing crucial information for diagnosis, management, and monitoring the acute responsiveness to intrapericardial chemotherapy. Immunocytochemistry (IHC) can identify specific markers for various types of cancer, enabling a more accurate diagnosis and guiding further treatment decisions.
Keywords: Thin Layer Cytology; ThinPrep; cardiac tamponade; immunocytochemistry; liquid based cytology; metastatic pericardial effusions.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Marcy P.Y., Magné N. Imaging of percutaneous pericardioperitoneal shunt in patient with malignant cardiac tamponade. JBR-BTR. 2004;87:186–189. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
