

Using Patient-Specific 3D-Printed C1-C2 Interfacet Spacers for the Treatment of Type 1 Basilar Invagination: A Clinical Case Report
- PMID: 40558377
- PMCID: PMC12190520
- DOI: 10.3390/biomimetics10060408
Using Patient-Specific 3D-Printed C1-C2 Interfacet Spacers for the Treatment of Type 1 Basilar Invagination: A Clinical Case Report
Abstract
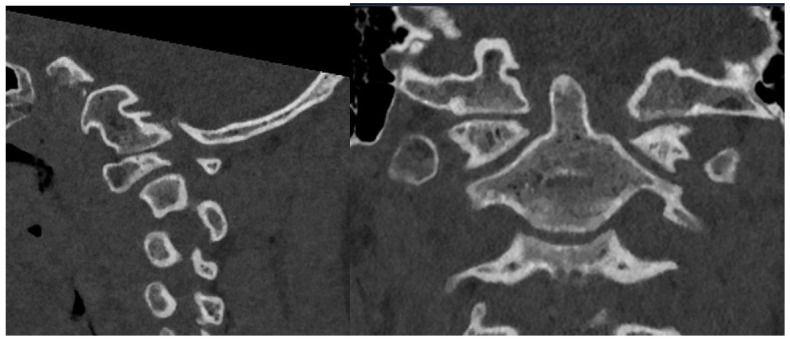
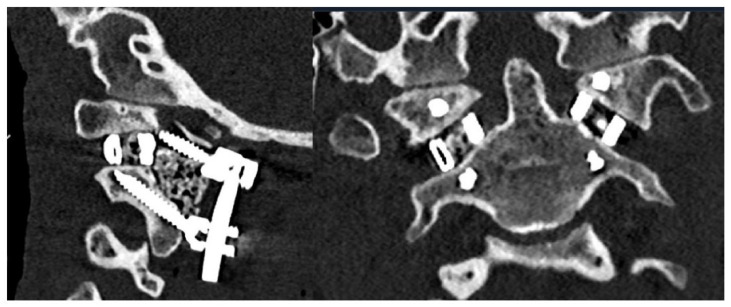
Background: Type 1 basilar invagination (BI) is caused by a structural instability at the craniovertebral junction (CVJ) and has been historically treated with distraction and stabilization through fusion of the C1-C2 vertebrae. Recent advances in 3D printed custom implants (3DPIs) have improved the array of available options for reaching distraction and alignment goals. Case Presentation: We report the case of a 15-year-old male who presented with early signs of cervical myelopathy. Radiographic evaluation revealed type 1 BI with a widened atlantodental interval (ADI) of 3.7 mm and a 9 mm McRae's line violation (MLV) of the dens, resulting in severe narrowing at the CVJ and brainstem/spinal cord impingement. Of note, the patient had bilateral dysplastic C1 and C2 anatomy, thus requiring a patient-specific 3DPI to conform to this anatomy and enable sufficient distraction and fusion. Custom 3D printed C1-C2 interfacet spacers were created and implemented within 14 days to achieve sufficient distraction, osteoconduction, and stabilization of the C1-C2 joint. Outcome: Postoperatively, the patient remained neurologically intact with myelopathic symptom improvement before discharge on postoperative day 4. Postoperative imaging demonstrated the resolution of BI from successful C1-C2 joint distraction and confirmed intended implant placement with resolution of canal stenosis. During his 6-week follow-up, the patient remained neurologically stable with intact hardware and preserved alignment. Conclusions: This case is the first in the United States demonstrating the use of custom 3D printed interfacet spacers to achieve successful distraction, decompression, and stabilization of type 1 BI. These patient-specific 3DPIs were designed and created in a streamlined manner and serve as proof-of-concept of pragmatic implant design and manufacturing. Future optimization of the workflow and characterization of long-term patient outcomes should be explored for these types of 3DPI.
Keywords: atlantoaxial instability; basilar invagination; cervical spine; craniovertebral junction; custom implant; pediatric spine; three-dimensional printing.
Conflict of interest statement
Authors report no relevant conflict of interests. C.A.M. is a consultant for Kuros, Augmedics, SMAIO, Baxter Health, and SI-Bone.
Figures







Similar articles
-
The importance of stabilisation in enabling bone fusion demonstrated by successful revision of failed occipitocervical fusion using patient-specific atlantoaxial joint spacers: a case report.J Spine Surg. 2025 Jun 27;11(2):354-362. doi: 10.21037/jss-24-157. Epub 2025 Jun 10. J Spine Surg. 2025. PMID: 40621374 Free PMC article.
-
Endoscopic Transnasal Approach to Atlantoaxial Decompression and C1-2 Fixation in Basilar Invagination of Adults: A Feasibility Study.Neurospine. 2025 Jun;22(2):543-555. doi: 10.14245/ns.2449320.660. Epub 2025 Jun 30. Neurospine. 2025. PMID: 40625015 Free PMC article.
-
Clinical and surgical characteristic of atlantoaxial reduction and fixation for patients with syringomyelia caused by atlantoaxial dislocation: retrospective study of 101 cases.Spine J. 2025 Jul;25(7):1418-1427. doi: 10.1016/j.spinee.2025.01.025. Epub 2025 Jan 31. Spine J. 2025. PMID: 39894270
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Surgical Treatment of Basilar Invagination without Evident Atlantoaxial Instability (Type B) - A Systematic Review.Neurol India. 2025 May 1;73(3):423-428. doi: 10.4103/neurol-india.Neurol-India-D-24-00457. Epub 2025 May 23. Neurol India. 2025. PMID: 40408569 Review.
References
-
- Donnally I.C., Munakomi S., Varacallo M.A. StatPearls. StatPearls Publishing; Treasure Island, FL, USA: 2025. Basilar Invagination. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
