

Cellular and Molecular Interactions in CNS Injury: The Role of Immune Cells and Inflammatory Responses in Damage and Repair
- PMID: 40558545
- PMCID: PMC12190931
- DOI: 10.3390/cells14120918
Cellular and Molecular Interactions in CNS Injury: The Role of Immune Cells and Inflammatory Responses in Damage and Repair
Abstract
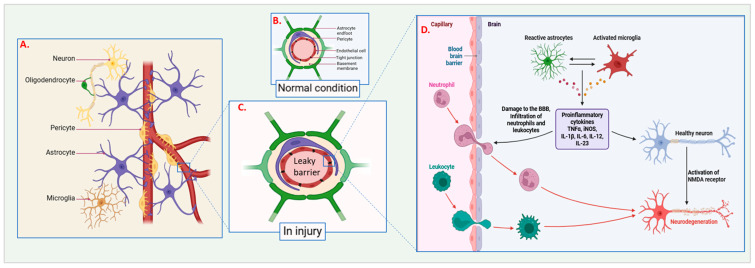
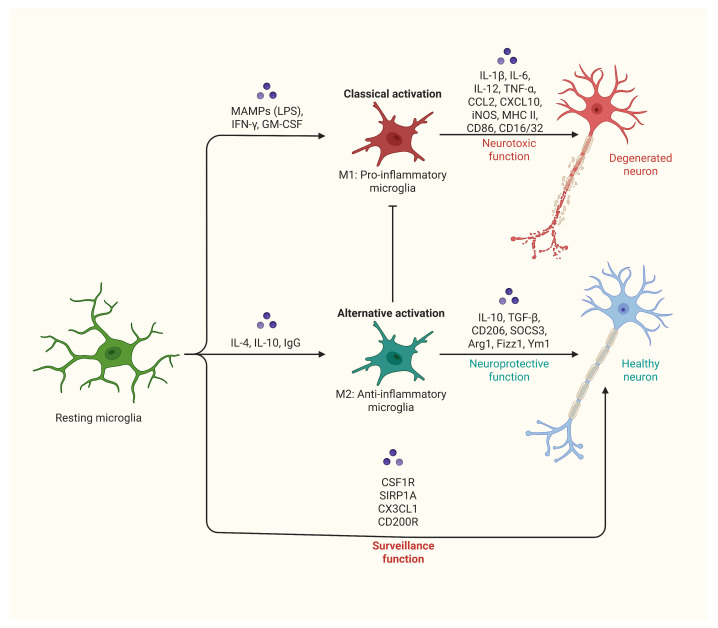
The central nervous system (CNS) is highly susceptible to damage due to its limited ability to regenerate. Injuries to the CNS, whether from trauma, ischemia, or neurodegenerative diseases, disrupt both cellular and vascular structures, leading to immediate (primary) and subsequent (secondary) damage. Primary damage involves the physical disruption of cells and blood vessels, weakening the blood-brain barrier (BBB) and triggering excitotoxicity and calcium overload. Secondary damage develops over hours to days and is marked by ionic imbalance, mitochondrial dysfunction, oxidative stress, and chronic inflammation, which further aggravates tissue damage. Inflammation plays a dual role: acute inflammation helps in repair, while chronic inflammation accelerates neurodegeneration. Microglia and astrocytes play key roles in this inflammatory response, with M1-like microglia promoting pro-inflammatory responses and M2-like microglia supporting anti-inflammatory and repair processes. Neurodegenerative diseases are characterized by the accumulation of misfolded proteins such as Tau, amyloid-beta, TDP-43, and α-synuclein, which impair cellular function and lead to neuronal loss. Neurodegenerative diseases are characterized by the accumulation of misfolded proteins and influenced by genetic risk factors (e.g., APOE4, TARDBP). Despite the CNS's limited regenerative abilities, processes like synaptogenesis, neurogenesis, axonal regeneration, and remyelination offer potential for recovery. Therapeutic approaches aim to target inflammatory pathways, enhance repair mechanisms, and develop neuroprotective treatments to counter excitotoxicity, oxidative stress, and apoptosis. Advances in stem cell therapy, gene therapy, and personalized medicine hold promise for improving outcomes. Future research should focus on combining strategies, utilizing advanced technologies, and conducting translational studies to bridge the gap between preclinical research and clinical application. By better understanding and leveraging the complex processes of CNS injury and repair, researchers hope to develop effective therapies to restore function and enhance the quality of life for individuals with CNS disorders.
Keywords: CNS injury; excitotoxicity; inflammation; microglia; neurodegenerative diseases; neurogenesis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Price L., Wilson C., Grant G. Blood-Brain Barrier Pathophysiology Following Traumatic Brain Injury. CRC Press; Boca Raton, FL, USA: 2016. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
