

A 10-Year Follow-Up of an Approach to Restore a Case of Extreme Erosive Tooth Wear
- PMID: 40559162
- PMCID: PMC12191467
- DOI: 10.3390/dj13060259
A 10-Year Follow-Up of an Approach to Restore a Case of Extreme Erosive Tooth Wear
Abstract
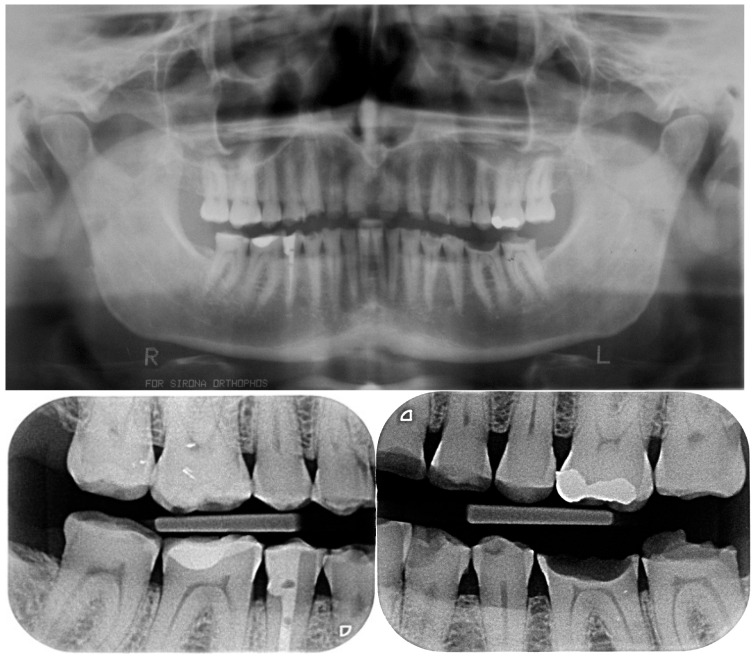
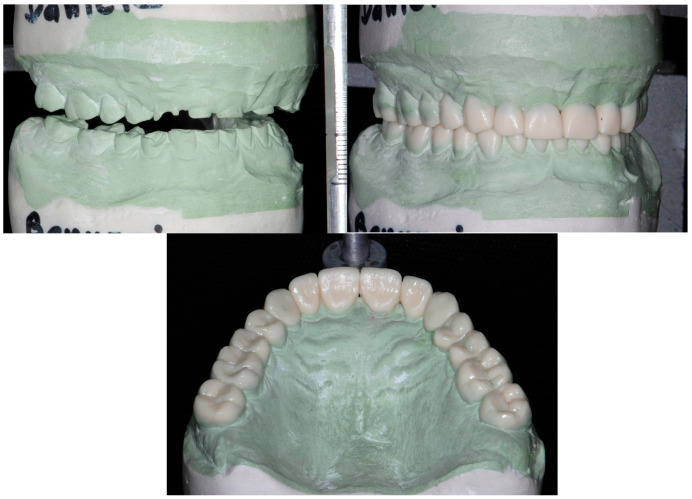
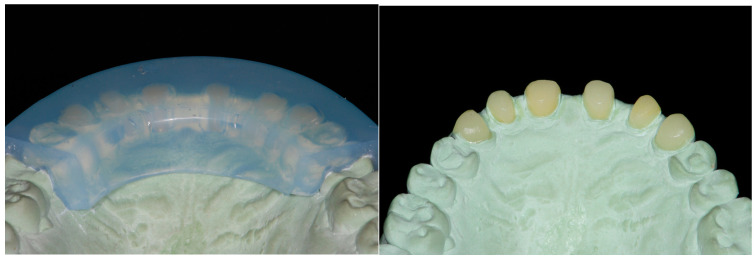
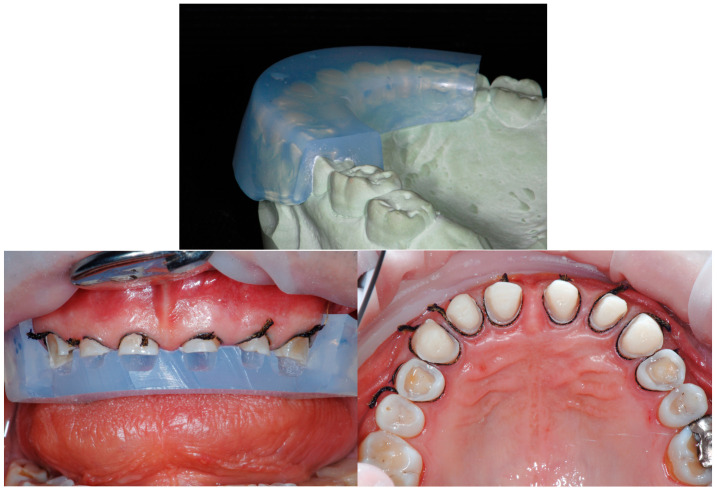
Background: In recent years, thanks to the improvement of adhesive techniques, patients affected by tooth wear, related to erosion and/or parafunctional habits, can undergo restoration by adding only what has been lost of their dentition (additive approach). However, since not all clinicians are convinced that dental rehabilitation should be proposed in the early stages of exposed dentin, several treatments are often postponed. It is important to emphasize that, in the early stages, the clinical approach should remain conservative, focusing on dietary counseling, the modification of harmful habits, fluoride application, and risk factor management. Only when these preventive and non-invasive strategies prove insufficient, and the condition continues to progress, should invasive restorative treatments be considered. Unfortunately, epidemiological studies are reporting an increase in the number of young patients affected by erosive tooth wear, and not intercepting these cases earlier could lead to a severe degradation of the affected dentition. In addition, parafunctional habits are also becoming more frequent among patients. The combination of erosion and attrition can be very destructive, and may progress rapidly once dentin is exposed and the risk factors remain unaddressed. The aim of this report was to present a conservative full-mouth rehabilitation approach for severe erosive lesions and to provide a 10-year follow-up assessing the biological, functional, and esthetic outcomes. Methods: In this article, the postponed restorative treatment of a patient, suffering from severe tooth wear, is illustrated. The patient had sought dental treatment in the past; however, due to the already very compromised dentition, a conventional but very aggressive treatment was proposed and refused. Four years later, when the patient finally accepted an alternative conservative therapy, the tooth degradation was very severe, especially at the level of the maxillary anterior teeth. The combination of three different approaches, Speed-Up Therapy, BOPT (Biologically-Oriented Preparation Technique), and the 3 Step Technique, however, improved the capacity to successfully complete the difficult therapeutic task. Results: The biological goals (maintenance of the pulp vitality of all of the teeth and the minimal removal of healthy tooth structure) were accomplished, relying only on adhesive techniques. Conclusions: The overall treatment was very comfortable for the patient and less complicated for the clinician. At 10-year follow-up, biological, functional, and esthetic success was still confirmed.
Keywords: full-mouth rehabilitation; mock-up; orthodontics; set-up; smile aesthetics; speed-up therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures































Similar articles
-
WITHDRAWN: Dental fillings for the treatment of caries in the primary dentition.Cochrane Database Syst Rev. 2016 Oct 17;10(10):CD004483. doi: 10.1002/14651858.CD004483.pub3. Cochrane Database Syst Rev. 2016. PMID: 27748505 Free PMC article.
-
Dental fillings for the treatment of caries in the primary dentition.Cochrane Database Syst Rev. 2009 Apr 15;(2):CD004483. doi: 10.1002/14651858.CD004483.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2016 Oct 17;10:CD004483. doi: 10.1002/14651858.CD004483.pub3. PMID: 19370602 Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Direct composite resin fillings versus amalgam fillings for permanent posterior teeth.Cochrane Database Syst Rev. 2021 Aug 13;8(8):CD005620. doi: 10.1002/14651858.CD005620.pub3. Cochrane Database Syst Rev. 2021. PMID: 34387873 Free PMC article.
References
-
- Hoek H.W., Vandereycken W. Eating disorders; 25 years of research and treatment. Tijdschr. Voor Psychiatr. 2008;50:85–89. - PubMed
-
- Sabahipour L., Bartlett D. A questionnaire based study to investigate the variations in the management of tooth wear by UK and prosthodontists from other countries. Eur. J. Prosthodont. Restor. Dent. 2009;17:61–66. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
