

Coverage Gaps and Contraceptive Use Among Medicare Enrollees With Disabilities
- PMID: 40560583
- PMCID: PMC12199052
- DOI: 10.1001/jamanetworkopen.2025.17718
Coverage Gaps and Contraceptive Use Among Medicare Enrollees With Disabilities
Abstract
Importance: Medicare is the primary health insurance payer for 1.5 million reproductive-aged women with disabilities, yet it is the only major form of US health insurance that is not required to cover contraceptives for pregnancy prevention.
Objective: To evaluate whether Medicare's contraceptive coverage gaps were associated with reduced use of contraceptives by enrollees with disabilities.
Design, setting, and participants: In this national, cross-sectional study, traditional Medicare (TM), Medicare Advantage (MA), and Medicaid claims from female enrollees aged 20 to 49 years receiving Social Security Disability Insurance or Supplemental Security Income from January 1, 2016, to December 31, 2020, were linked. The propensity score-weighted probability of contraceptive use by public insurance type was estimated, then the association between gaining contraceptive coverage through a transition from Medicare to dual Medicare-Medicaid enrollment and contraceptive use was evaluated using a staggered-entry difference-in-differences design. Data were analyzed from December 3, 2024, to April 5, 2025.
Exposures: Public insurance enrollment in TM, MA, dual TM-Medicaid, dual MA-Medicaid, or Medicaid.
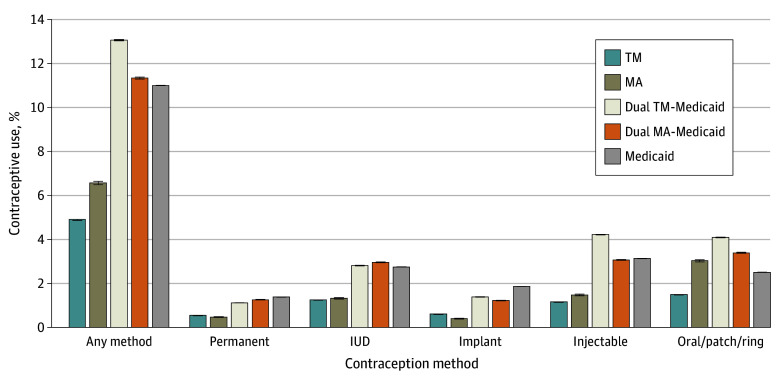
Main outcomes and measures: Monthly use of permanent contraceptives, long-acting reversible contraceptives (intrauterine device and implant), and short-acting contraceptives (injectable and oral contraceptives, patch, and ring).
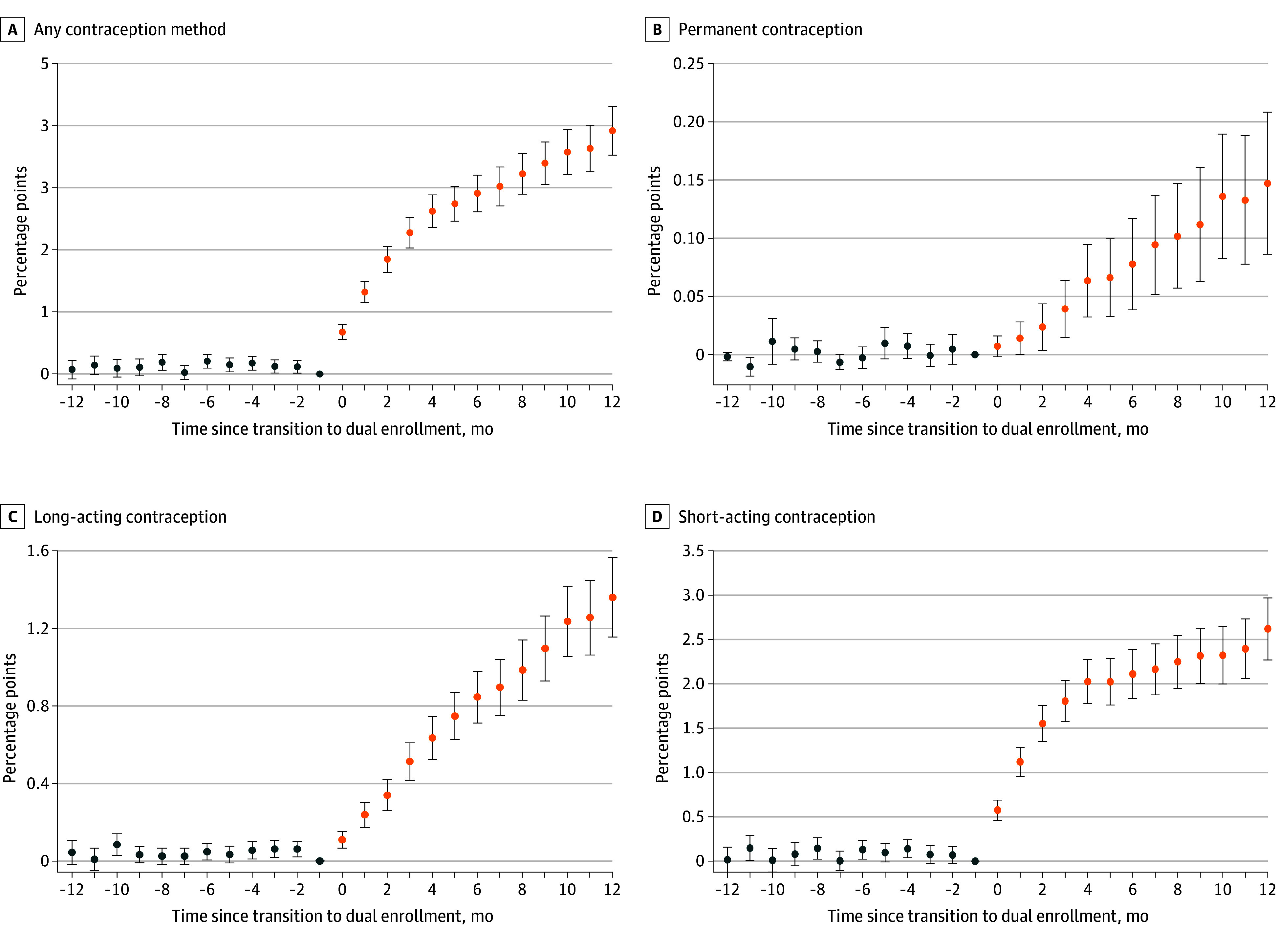
Results: A total of 51 501 303 monthly observations from 1 606 129 women were included in the analysis. Mean (SD) age was 35.93 (8.58) years; 1.8% of monthly observations were from Asian women, 30.7% from Black women, 13.0% from Hispanic women, 52.6% from White women, and 1.9% from multiracial women or women identifying as another race and ethnicity not reported on previously. Those enrolled in TM and MA were more often older and non-Hispanic White compared with those dual enrolled or enrolled in Medicaid. The estimated monthly probability of use of any contraceptive method was lowest among TM (4.9%; 95% CI, 4.9%-4.9%) and MA (6.6%; 95% CI, 6.5%-6.6%) enrollees, followed by Medicaid (11.0%; 95% CI, 11.0%-11.0%), dual MA-Medicaid (11.3%; 95% CI, 11.3%-11.4%), and dual TM-Medicaid (13.1%; 95% CI, 13.0%-13.1%) enrollees. Gaining contraceptive coverage through dual enrollment was associated with an increase of 3.9 (95% CI, 3.5-4.3) percentage points (35%) in use of any contraceptive method, with the largest increase in use of short-acting methods at 2.6 (95% CI, 2.3-3.0) percentage points (45%).
Conclusions and relevance: In this cross-sectional study of contraceptive use in the Medicare program, gaining contraceptive coverage through dual Medicare-Medicaid enrollment was associated with increased contraceptive use among disabled Medicare enrollees, suggesting that Medicare's coverage gaps pose a financial barrier to desired contraceptive use. Given these findings, Medicare should be required to cover all US Food and Drug Administration-approved contraceptive methods without cost-sharing. Doing so would align Medicare's coverage requirements with those of Medicaid, private insurance plans, and TRICARE.
Conflict of interest statement
Figures
Comment in
- doi: 10.1001/jamanetworkopen.2025.17729
Similar articles
-
Quality of Hospices Used by Medicare Advantage and Traditional Fee-for-Service Beneficiaries.JAMA Netw Open. 2024 Dec 2;7(12):e2451227. doi: 10.1001/jamanetworkopen.2024.51227. JAMA Netw Open. 2024. PMID: 39680405 Free PMC article.
-
Racial and Ethnic Disparities in Health Care Use and Access Associated With Loss of Medicaid Supplemental Insurance Eligibility Above the Federal Poverty Level.JAMA Intern Med. 2023 Jun 1;183(6):534-543. doi: 10.1001/jamainternmed.2023.0512. JAMA Intern Med. 2023. PMID: 37036727 Free PMC article.
-
Outcomes for Dual-Eligible Beneficiaries With Dementia in Special Needs Plans and Other Medicare Advantage Plans.JAMA Netw Open. 2025 Feb 3;8(2):e2461219. doi: 10.1001/jamanetworkopen.2024.61219. JAMA Netw Open. 2025. PMID: 39982721 Free PMC article.
-
Risk of thromboembolism in patients with COVID-19 who are using hormonal contraception.Cochrane Database Syst Rev. 2023 Jan 9;1(1):CD014908. doi: 10.1002/14651858.CD014908.pub2. Cochrane Database Syst Rev. 2023. Update in: Cochrane Database Syst Rev. 2023 May 15;5:CD014908. doi: 10.1002/14651858.CD014908.pub3. PMID: 36622724 Free PMC article. Updated.
-
Steroidal contraceptives and bone fractures in women: evidence from observational studies.Cochrane Database Syst Rev. 2012 Aug 15;(8):CD009849. doi: 10.1002/14651858.CD009849.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 Jul 21;(7):CD009849. doi: 10.1002/14651858.CD009849.pub3. PMID: 22895991 Updated.
References
-
- Frederiksen B, Diep K, Salganicoff A. Contraceptive experiences, coverage, and preferences: findings from the 2024 KFF Women’s Health Survey. November 22, 2024. Accessed December 23, 2024. https://www.kff.org/womens-health-policy/issue-brief/contraceptive-exper...
-
- PBS . A timeline of contraception. The American Experience Trust. Accessed December 23, 2024. https://www.pbs.org/wgbh/americanexperience/features/pill-timeline/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
