

Intraosseous vs Intravenous Access for Epinephrine in Pediatric Out-of-Hospital Cardiac Arrest
- PMID: 40560587
- PMCID: PMC12199053
- DOI: 10.1001/jamanetworkopen.2025.17291
Intraosseous vs Intravenous Access for Epinephrine in Pediatric Out-of-Hospital Cardiac Arrest
Abstract
Importance: While epinephrine is commonly administered in children with out-of-hospital cardiac arrest (OHCA) via an intraosseous (IO) or intravenous (IV) route, the optimal route of epinephrine delivery is unclear.
Objective: To evaluate the association between the route of epinephrine administration (IO or IV) and patient outcomes after pediatric OHCA.
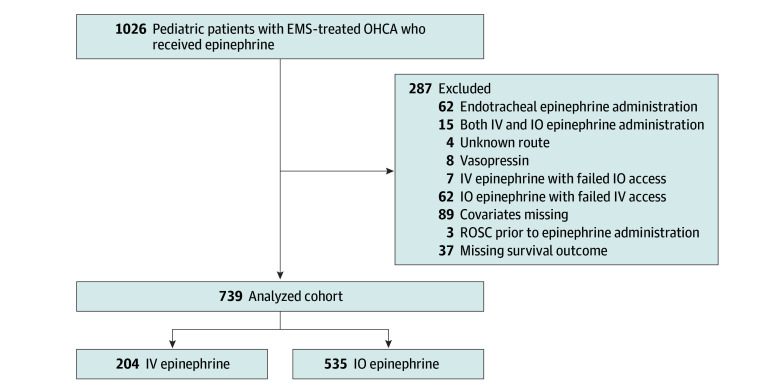
Design, setting, and participants: Retrospective cohort study of pediatric patients (aged <18 years) with nontraumatic OHCA treated by emergency medical services who received prehospital epinephrine either via an IO or IV route. Patients were included in the Resuscitation Outcomes Consortium Epidemiologic Registry, a prospective OHCA registry at 10 sites in the US and Canada from April 2011 to June 2015. Data analysis was performed from May 2024 to April 2025.
Exposure: Epinephrine administration route: IO or IV route.
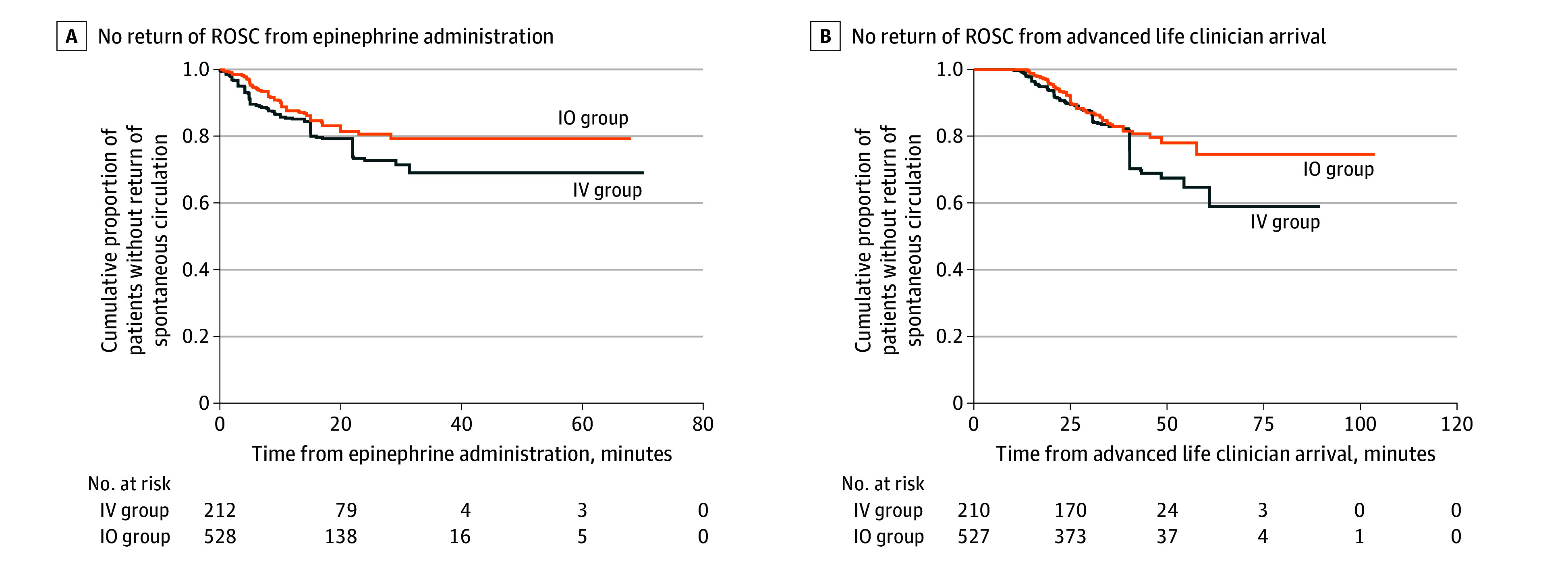
Main outcomes and measures: The primary outcome was survival to hospital discharge. The secondary outcome was return of spontaneous circulation (ROSC) before hospital arrival. Propensity scores were calculated and inverse probability of treatment weighting (IPTW) was performed with stabilized weights to control imbalances in measured patient demographics, cardiac arrest characteristics, and bystander and prehospital interventions.
Results: Of 739 eligible patients (median [IQR] age, 1 [0-11] years), 449 (60.8%) were male. Epinephrine was administered via an IO route for 535 (72.4%) and via an IV route for 204 (27.6%) patients. In the IPTW pseudopopulation (740 weighted cases), there was no significant difference in survival to hospital discharge (IO epinephrine: 28 of 528 patients [5.3%] vs IV epinephrine: 12 of 212 patients [5.7%]; risk ratio [RR], 0.92; 95% CI, 0.41-2.07) or prehospital ROSC (IO epinephrine: 76 of 528 patients [14.4%] vs IV epinephrine: 46 of 212 patients [21.7%]; RR, 0.66; 95% CI, 0.42-1.03) between the IO and IV epinephrine groups.
Conclusions and relevance: In this retrospective cohort study of pediatric patients with OHCA in the US and Canada, the route of epinephrine administration was not associated with survival to hospital discharge or prehospital ROSC. This may support the practice of administering epinephrine via IO or IV route.
Conflict of interest statement
Figures
References
-
- Topjian AA, Raymond TT, Atkins D, et al. ; Pediatric Basic and Advanced Life Support Collaborators . Part 4: pediatric basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2)(suppl 2):S469-S523. doi: 10.1161/CIR.0000000000000901 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
