

Developing Machine-Learning Models to Predict Bacteremia in Febrile Adults Presenting to the Emergency Department: A Retrospective Cohort Study from a Large Center
- PMID: 40562007
- PMCID: PMC12208070
- DOI: 10.5811/westjem.35866
Developing Machine-Learning Models to Predict Bacteremia in Febrile Adults Presenting to the Emergency Department: A Retrospective Cohort Study from a Large Center
Abstract
Introduction: Bacteremia, a common disease but difficult to diagnose early, may result in significant morbidity and mortality without prompt treatment. We aimed to develop machine-learning (ML) algorithms to predict patients with bacteremia from febrile patients presenting to the emergency department (ED) using data that is readily available at the triage.
Methods: We included all adult patients (≥18 years of age) who presented to the emergency department (ED) of National Taiwan University Hospital (NTUH), a tertiary teaching hospital in Taiwan, with the chief complaint of fever or measured body temperature more than 38°C, and who received at least one blood culture during the ED encounter. We extracted data from the Integrated Medical Database of NTUH from 2009-2018.The dataset included patient demographics, triage details, symptoms, and medical history. The positive blood culture result of at least one potential pathogen was defined as bacteremia and used as the binary classification label. We split the dataset into training/validation and testing sets (60-to-40 ratio) and trained five supervised ML models using K-fold cross-validation. The model performance was evaluated using the area under the receiver operating characteristic curve (AUC) in the testing set.
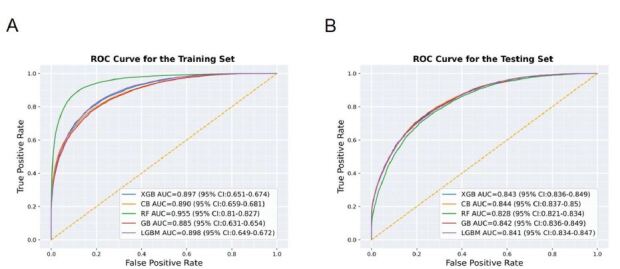
Results: We included 80,201 cases in this study. Of them, 48120 cases were assigned to the training/validation set and 32,081 to the testing set. Bacteremia was identified in 5,831 (12.1%) and 3,824 (11.9%) cases of the training/validation set and test set, respectively. All ML models performed well, with CatBoost achieving the highest AUC (.844, 95% confidence interval [CI] .837-.850), followed by extreme gradient boosting (.843, 95% CI .836-.849), gradient boosting (.842, 95% CI .836-.849), light gradient boosting machine (.841, 95% CI .834-.847), and random forest (.828, 95% CI .821-.834).
Conclusion: Our machine-learning model has shown excellent discriminatory performance to predict bacteremia based only on clinical features at ED triage. It has the potential to improve care quality and save more lives if successfully implemented in the ED.
Conflict of interest statement
Figures


Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
A web-based tool utilizing machine learning algorithms for predicting illicit drug use in emergency departments.Int J Med Inform. 2025 Nov;203:106031. doi: 10.1016/j.ijmedinf.2025.106031. Epub 2025 Jun 30. Int J Med Inform. 2025. PMID: 40618645
-
Prediction of Insulin Resistance in Nondiabetic Population Using LightGBM and Cohort Validation of Its Clinical Value: Cross-Sectional and Retrospective Cohort Study.JMIR Med Inform. 2025 Jun 13;13:e72238. doi: 10.2196/72238. JMIR Med Inform. 2025. PMID: 40512995 Free PMC article.
-
Supervised Machine Learning Models for Predicting Sepsis-Associated Liver Injury in Patients With Sepsis: Development and Validation Study Based on a Multicenter Cohort Study.J Med Internet Res. 2025 May 26;27:e66733. doi: 10.2196/66733. J Med Internet Res. 2025. PMID: 40418571 Free PMC article.
-
Systematic review and validation of prediction rules for identifying children with serious infections in emergency departments and urgent-access primary care.Health Technol Assess. 2012;16(15):1-100. doi: 10.3310/hta16150. Health Technol Assess. 2012. PMID: 22452986 Free PMC article.
References
-
- Søgaard M, Nørgaard M, Dethlefsen C, et al. Temporal changes in the incidence and 30-day mortality associated with bacteremia in hospitalized patients from 1992 through 2006: a population-based cohort study. Clin Infect Dis. 2011 Jan;52:61–9. - PubMed
-
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19:501–9. - PubMed
-
- Fabre V, Sharara SL, Salinas AB, et al. Does this patient need blood cultures? A scoping review of indications for blood cultures in adult nonneutropenic inpatients. Clin Infect Dis. 2020;71:1339–47. - PubMed
-
- Epstein D, Raveh D, Schlesinger Y, et al. Adult patients with occult bacteremia discharged from the emergency department: epidemiological and clinical characteristics. Clin Infect Dis. 2001;32:559–65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical