

Comparative Analysis of the ABC/2 Score and e-ASPECTS Software in the Determination of Acute Ischaemic Stroke Volume from Non-Contrast CT
- PMID: 40563732
- PMCID: PMC12190421
- DOI: 10.3390/brainsci15060560
Comparative Analysis of the ABC/2 Score and e-ASPECTS Software in the Determination of Acute Ischaemic Stroke Volume from Non-Contrast CT
Abstract
Background and purpose: Accurate and reproducible methods for assessing infarct volume in acute ischaemic stroke have important therapeutic and prognostic implications for the choice and success of acute therapeutic interventions. However, there is no international consensus on the methodology employed in infarct volume assessment. We aimed to assess the reliability of the ABC/2 score and e-ASPECTS in the determination of infarct volume in acute ischaemic stroke.
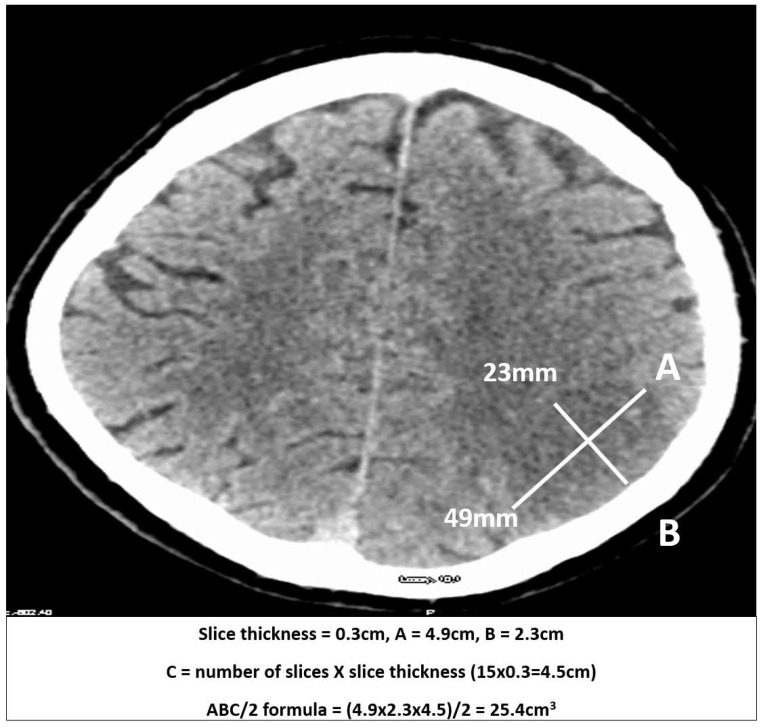
Methods: Infarct volume was measured from NCCT in stroke patients recruited ≤12 h of symptoms onset and at 24 h using the ABC/2 method. Automated ischaemic volume measurements were carried out using e-ASPECTS software. Measurements using ABC/2 were compared with e-ASPECTS to assess volume differences and reliability using Lin's concordance correlation coefficient.
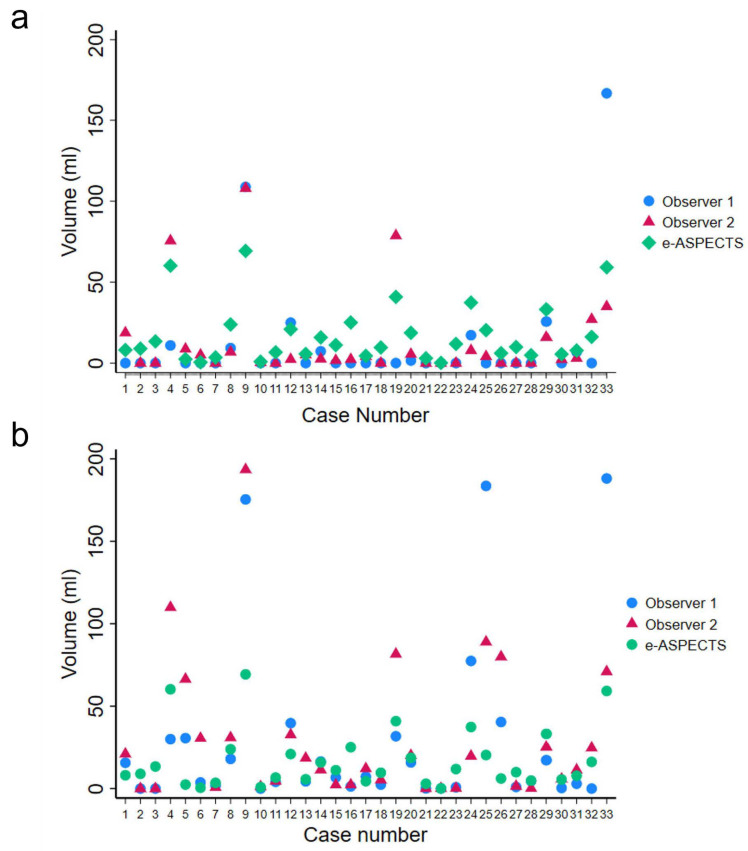
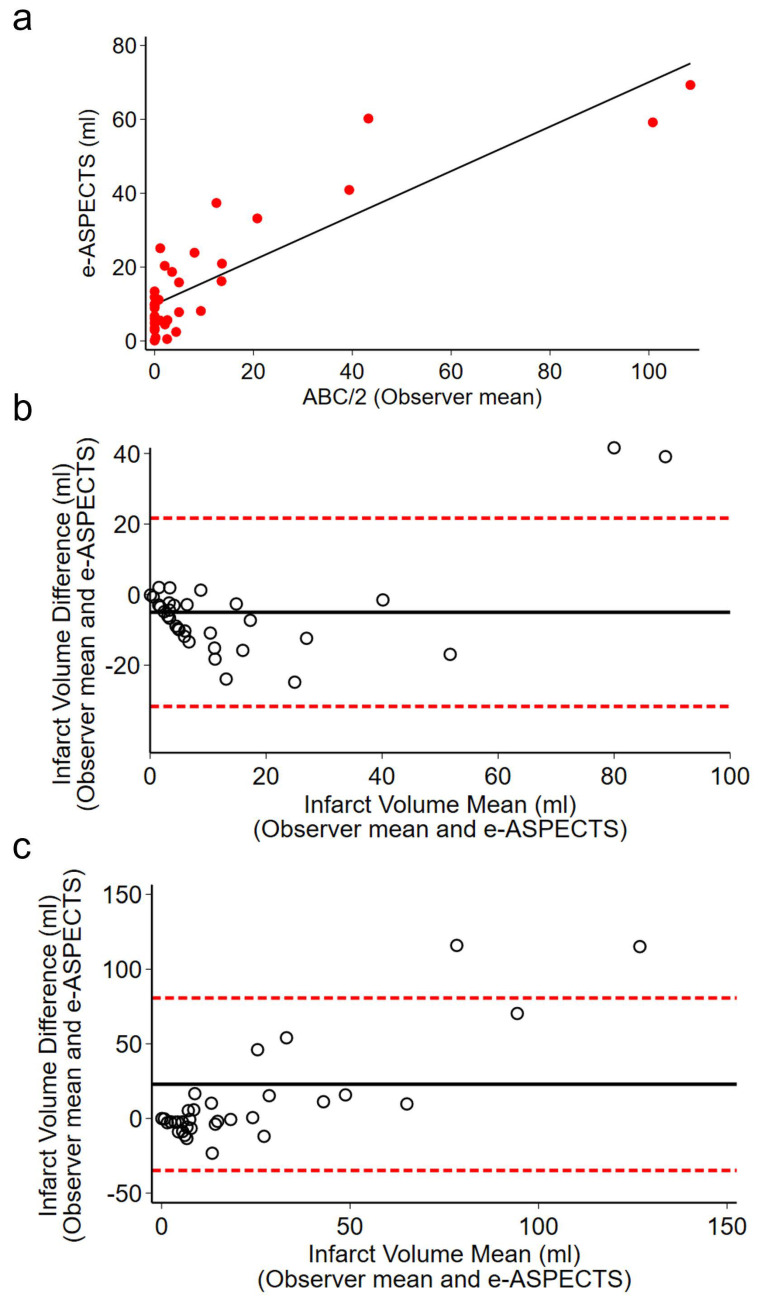
Results: Thirty-three patients with CT < 12 h from onset of symptoms and follow-up at 24 h were included in the analysis. Use of ABC/2 demonstrated low agreement between observers (0.490, CI 0.236-0.743, p < 0.001) on admission (<12 h). High agreement was found between observers at 24 h (0.724, CI 0.564-0.884, p < 0.001). High agreement was observed between the mean observed infarct volumes using ABC/2 and e-ASPECTS on admission (0.794, CI 0.691-0.898, p < 0.001).
Conclusions: Our results suggest that e-ASPECTS is a reliable platform for ischaemic volume determination particularly in the hyperacute phase to inform management. However, the use of ABC/2 represents an alternative approach to e-ASPECTS in the rapid and reliable estimation of ischaemic infarct volume to inform prognosis and treatment decisions, particularly in cases of delayed presentation where infarction is established and arterial territory boundaries are easily identifiable.
Keywords: ABC/2; infarct measurement; infarct volume; ischaemic stroke; non-contrast computerised tomography; stroke.
Conflict of interest statement
O.J. is employed at Brainomix, UK. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Figures
References
-
- Ospel J.M., Hill M.D., Menon B.K., Demchuk A., McTaggart R., Nogueira R., Poppe A., Haussen D., Qiu W., Mayank A., et al. Strength of Association between Infarct Volume and Clinical Outcome Depends on the Magnitude of Infarct Size: Results from the ESCAPE-NA1 Trial. Am. J. Neuroradiol. 2021;42:1375–1379. doi: 10.3174/ajnr.A7183. - DOI - PMC - PubMed
-
- Boers A.M.M., Jansen I.G.H., Brown S., Lingsma H.F., Beenen L.F.M., Devlin T.G., Román L.S., Heo J.-H., Ribó M., Almekhlafi M.A., et al. Mediation of the Relationship Between Endovascular Therapy and Functional Outcome by Follow-up Infarct Volume in Patients With Acute Ischemic Stroke. JAMA Neurol. 2019;76:194–202. doi: 10.1001/jamaneurol.2018.3661. - DOI - PMC - PubMed
-
- Albers G.W., Marks M.P., Kemp S., Christensen S., Tsai J.P., Ortega-Gutierrez S., McTaggart R.A., Torbey M.T., Kim-Tenser M., Leslie-Mazwi T., et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018;378:708–718. doi: 10.1056/NEJMoa1713973. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
