

Atherosclerosis and Insulin Resistance: Is There a Link Between Them?
- PMID: 40564010
- PMCID: PMC12189823
- DOI: 10.3390/biomedicines13061291
Atherosclerosis and Insulin Resistance: Is There a Link Between Them?
Abstract
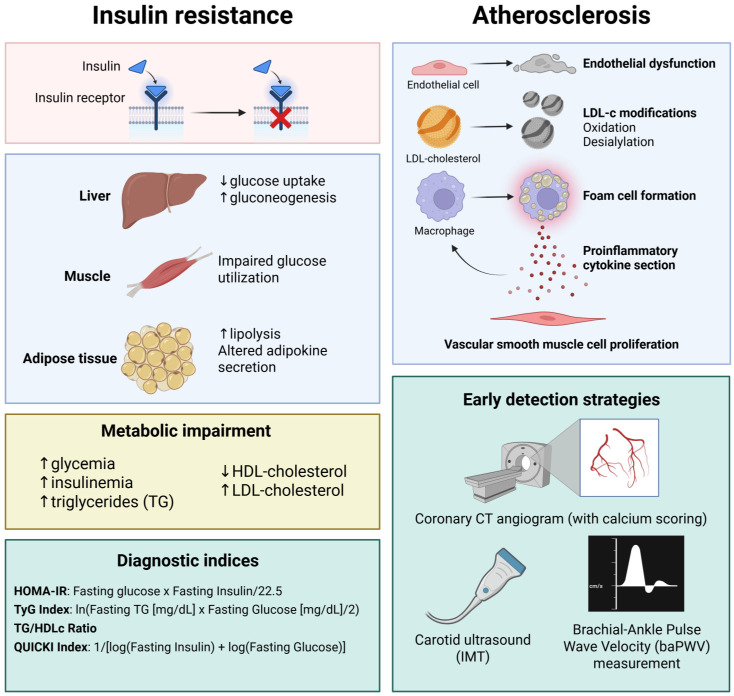
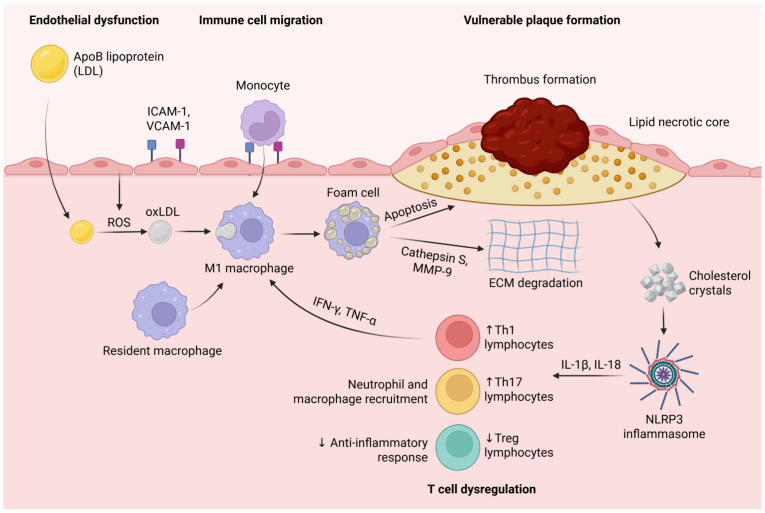
Cardiovascular disease remains the leading cause of morbidity and mortality worldwide, especially in regions like Eastern Europe, South Asia, and Latin America. A significant portion of these cases (80%) is linked to atherosclerosis, which can lead to severe conditions like ischemic heart disease and stroke, with atherosclerosis (ATS) responsible for the majority of cases. This review explores the multifaceted relationship between insulin resistance (IR) and ATS, highlighting their roles as both independent and interrelated contributors to cardiovascular risk. ATS is characterized by lipid accumulation and chronic inflammation within arterial walls, driven by factors such as hypertension, dyslipidemia, and genetic predisposition, with endothelial dysfunction as a key early event. The early detection of subclinical ATS is critical and can be achieved through a combination of non-invasive imaging techniques-such as coronary artery calcium scoring and carotid ultrasound-and comprehensive risk profiling. IR, marked by impaired glucose uptake in liver, muscle, and adipose tissue, often precedes early diabetes and is associated with metabolic disturbances, including dyslipidemia and chronic inflammation. The diagnosis of IR relies on surrogate indices such as HOMA-IR, the QUICKI, and the TyG index, which facilitate screening in clinical practice. Compelling evidence indicates that IR independently predicts the progression of atherosclerotic plaques, even in non-diabetic individuals, and operates through both traditional risk factors and direct vascular effects. Understanding and targeting the IR-ATS axis is essential for the effective prevention and management of cardiovascular disease.
Keywords: cardiovascular risk; endothelial dysfunction; insulin resistance; subclinical atherosclerosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Vos T., Lim S.S., Abbafati C., Abbas K.M., Abbasi M., Abbasifard M., Abbasi-Kangevari M., Abbastabar H., Abd-Allah F., Abdelalim A., et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–1222. doi: 10.1016/S0140-6736(20)30925-9. - DOI - PMC - PubMed
-
- Fakhrzadeh H., Sharifi F., Alizadeh M., Arzaghi S.M., Tajallizade-Khoob Y., Tootee A., Benetos A., Biffi A., Boavida J.-M., Capodanno D., et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021;42:3227–3337. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
