

Real-World Efficacy of Minimally Invasive Revascularization in Diabetic Foot Ischemia: Impact of Device Selection and Lesion-Specific Factors
- PMID: 40564104
- PMCID: PMC12189699
- DOI: 10.3390/biomedicines13061384
Real-World Efficacy of Minimally Invasive Revascularization in Diabetic Foot Ischemia: Impact of Device Selection and Lesion-Specific Factors
Abstract
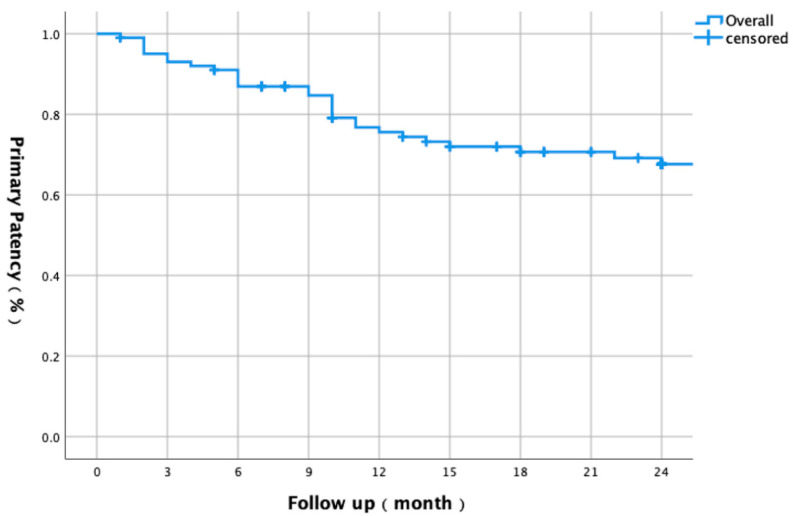
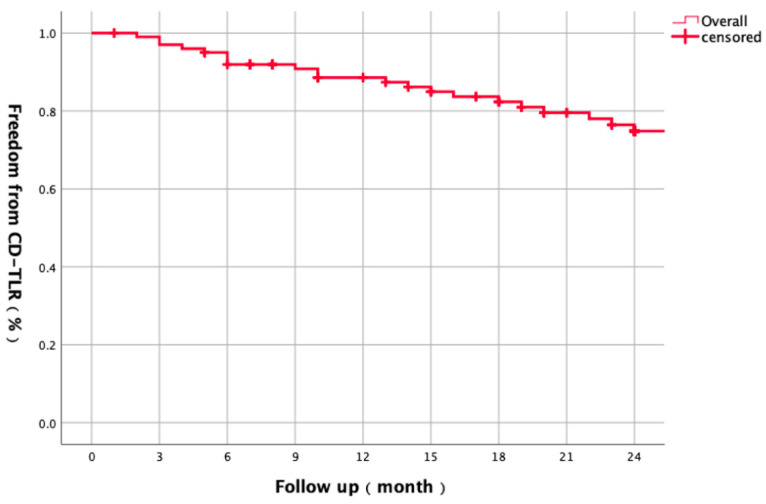
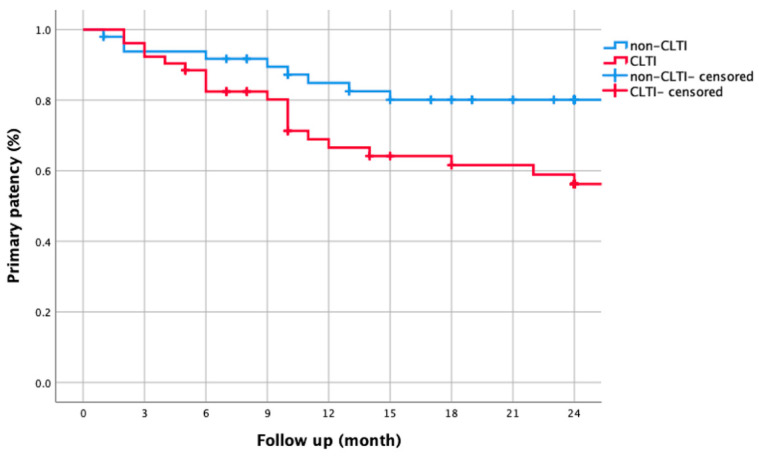
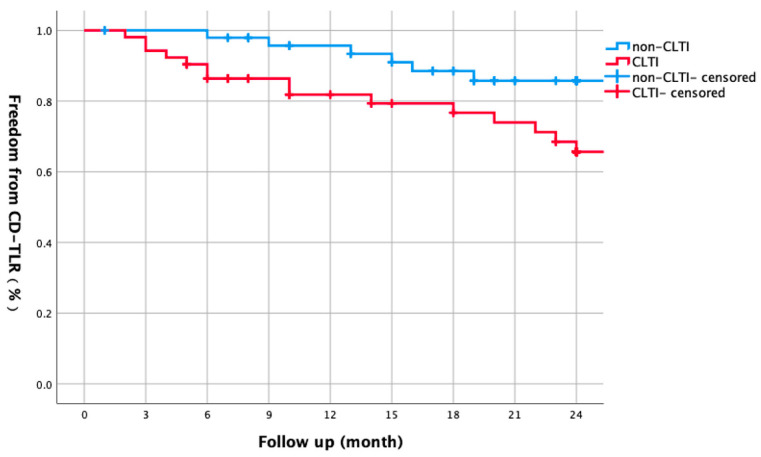
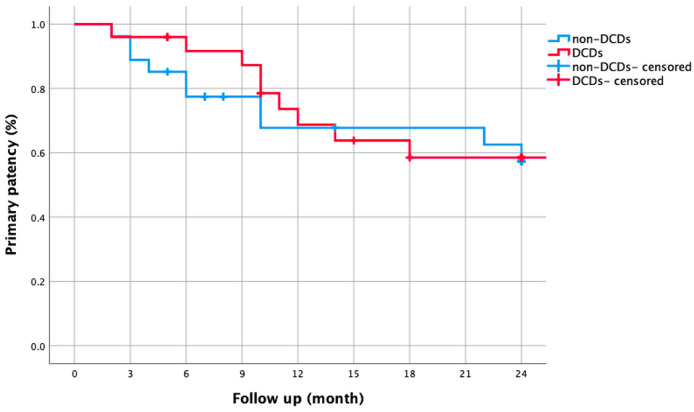
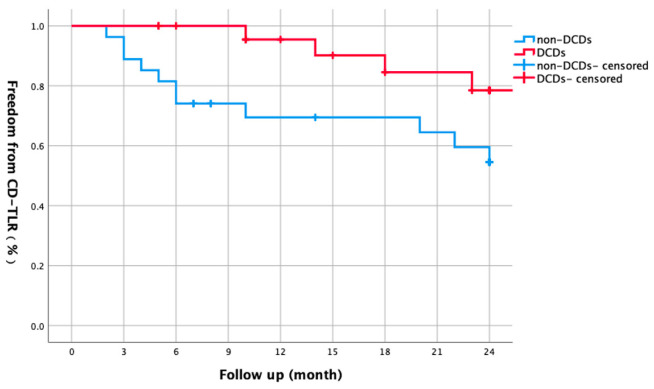
Objectives: The objective of this study was to evaluate the real-world efficacy of minimally invasive revascularization in diabetic foot ischemia, focusing on novel insights into device selection and lesion-specific predictors. Methods: This retrospective study included 98 patients (101 limbs) undergoing endovascular/hybrid interventions. The primary endpoints were 1- and 2-year primary patency and freedom from clinically driven target lesion revascularization (CD-TLR). Multivariate Cox regression identified restenosis predictors, with subgroup analysis comparing drug-coated devices (DCDs) versus conventional strategies in chronic limb-threatening ischemia (CLTI). Results: The cohort (mean age 72.1 ± 8.9 years) comprised 51% CLTI limbs (28.5% with tissue loss). The overall 1-year primary patency was 75.6%, declining to 67.6% after 2 years. The rates of freedom from CD-TLR were 87.4% after 1 year and 74.8% after 2 years. CLTI was associated with significantly reduced 1-year (66.5% vs. 84.9%) and 2-year primary patency (56.3% vs. 80.1%; log-rank p = 0.026) compared to non-CLTI. Multivariate analysis identified CLTI as an independent predictor of restenosis (HR 3.375, 95%CI 1.267-8.990, p = 0.015). Although DCDs did not improve 2-year primary patency in CLTI (58.5% vs. 57.3%, p = 0.768), they demonstrated superior 2-year CD-TLR-free survival (78.5% vs. 54.6%, p = 0.048). The total complication rate was 5.9%, with no significant difference between CLTI and non-CLTI groups (11.5% vs. 0%, p = 0.057). Conclusions: This study highlights CLTI's impact on revascularization durability and the clinical benefits of DCDs in reducing reinterventions, offering evidence-based insights for tailored device selection despite retrospective limitations.
Keywords: CLTI; PAD; diabetic foot ischemia; patency; revascularization.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Drug-eluting balloon angioplasty versus uncoated balloon angioplasty for peripheral arterial disease of the lower limbs.Cochrane Database Syst Rev. 2016 Aug 4;2016(8):CD011319. doi: 10.1002/14651858.CD011319.pub2. Cochrane Database Syst Rev. 2016. PMID: 27490003 Free PMC article.
-
A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia.J Vasc Surg. 2018 Aug;68(2):624-633. doi: 10.1016/j.jvs.2018.01.066. Epub 2018 May 24. J Vasc Surg. 2018. PMID: 29804736
-
Clinical outcomes in patients with chronic limb-threatening ischemia after femoropopliteal intervention with a drug-coated balloon or stenting.J Vasc Surg. 2025 Jul;82(1):164-172.e2. doi: 10.1016/j.jvs.2025.02.010. Epub 2025 Feb 18. J Vasc Surg. 2025. PMID: 39978489
-
Sciatic nerve atrophy as a risk factor for impaired wound healing in patients with chronic limb-threatening ischemia.J Vasc Surg. 2025 Jul;82(1):186-192.e1. doi: 10.1016/j.jvs.2025.02.008. Epub 2025 Feb 17. J Vasc Surg. 2025. PMID: 39971142
-
Graft type for femoro-popliteal bypass surgery.Cochrane Database Syst Rev. 2018 Feb 11;2(2):CD001487. doi: 10.1002/14651858.CD001487.pub3. Cochrane Database Syst Rev. 2018. PMID: 29429146 Free PMC article.
References
-
- Aiello A., Anichini R., Brocco E., Caravaggi C., Chiavetta A., Cioni R., Da Ros R., De Feo M., Ferraresi R., Florio F., et al. Treatment of peripheral arterial disease in diabetes: A consensus of the Italian Societies of Diabetes (SID, AMD), Radiology (SIRM) and Vascular Endovascular Surgery (SICVE) Nutr. Metab. Cardiovasc. Dis. 2014;24:355–369. doi: 10.1016/j.numecd.2013.12.007. - DOI - PubMed
-
- Morbach S., Furchert H., Gröblinghoff U., Hoffmeier H., Kersten K., Klauke G.-T., Klemp U., Roden T., Icks A., Haastert B., et al. Long-term prognosis of diabetic foot patients and their limbs: Amputation and death over the course of a decade. Diabetes Care. 2012;35:2021–2027. doi: 10.2337/dc12-0200. - DOI - PMC - PubMed
-
- Liistro F., Porto I., Angioli P., Grotti S., Ricci L., Ducci K., Falsini G., Ventoruzzo G., Turini F., Bellandi G., et al. Drug-eluting balloon in peripheral intervention for below the knee angioplasty evaluation (DEBATE-BTK): A randomized trial in diabetic patients with critical limb ischemia. Circulation. 2013;128:615–621. doi: 10.1161/CIRCULATIONAHA.113.001811. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
