

Point-of-Care Ultrasound Use in Hemodynamic Assessment
- PMID: 40564145
- PMCID: PMC12189778
- DOI: 10.3390/biomedicines13061426
Point-of-Care Ultrasound Use in Hemodynamic Assessment
Abstract
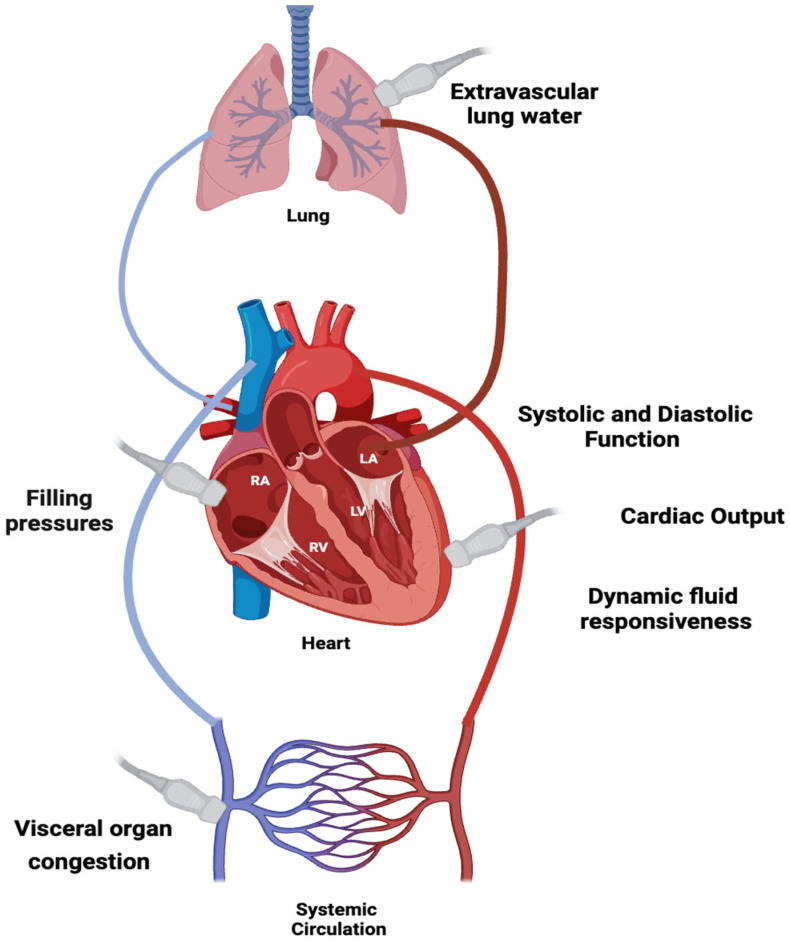
Hemodynamic assessment is critical in emergency and critical care for preventing, diagnosing, and managing shock states that significantly affect patient outcomes. Point-of-care ultrasound (POCUS) has become an invaluable, non-invasive, real-time, and reproducible tool for bedside decision-making. Advancements such as Doppler imaging, advanced critical care ultrasonography, and transesophageal echocardiography (TEE) have expanded its utility, enabling rapid and repeatable evaluations, especially in complex mixed shock presentations. This review explores the role of POCUS in hemodynamic monitoring, emphasizing its ability to assess cardiac output, filling pressures, and vascular congestion, facilitating shock classification and guiding fluid management. We highlight an extensive array of POCUS techniques for evaluating right and left cardiac function and review existing literature on their advantages, limitations, and appropriate clinical applications. Beyond assessing volume status, this review discusses the role of POCUS in predicting fluid responsiveness and supporting more individualized, precise management strategies. Ultimately, while POCUS is a powerful tool for rapid, comprehensive hemodynamic assessment in acute settings, its limitations must be acknowledged and thoughtfully integrated into clinical decision-making.
Keywords: cardiac arrest; critical care; echocardiography; emergency medicine; hemodynamics; point of care; ultrasound; volume assessment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
