

A Word of Caution-Potential Limitations of Pulmonary Artery Pressure Monitoring in Detecting Congestion Caused by Right-Sided Heart Failure
- PMID: 40564188
- PMCID: PMC12190875
- DOI: 10.3390/biomedicines13061469
A Word of Caution-Potential Limitations of Pulmonary Artery Pressure Monitoring in Detecting Congestion Caused by Right-Sided Heart Failure
Abstract
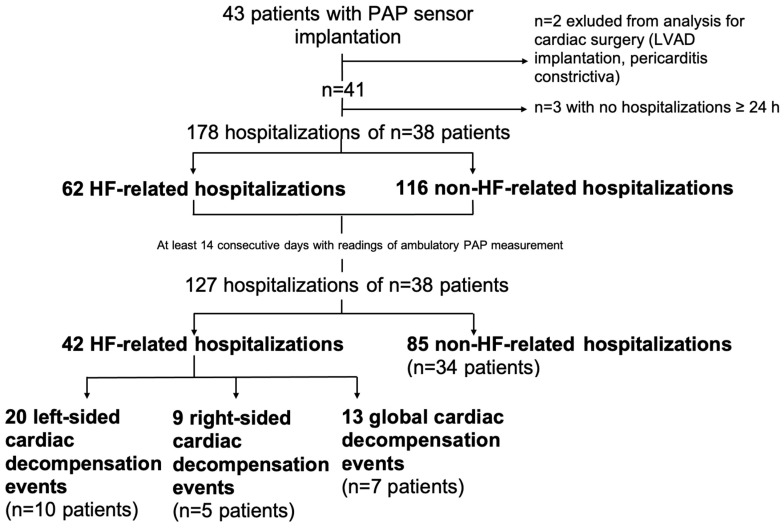
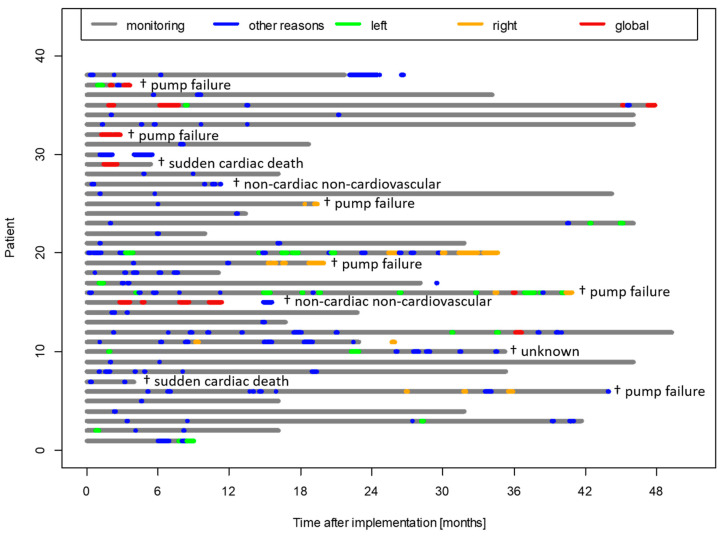
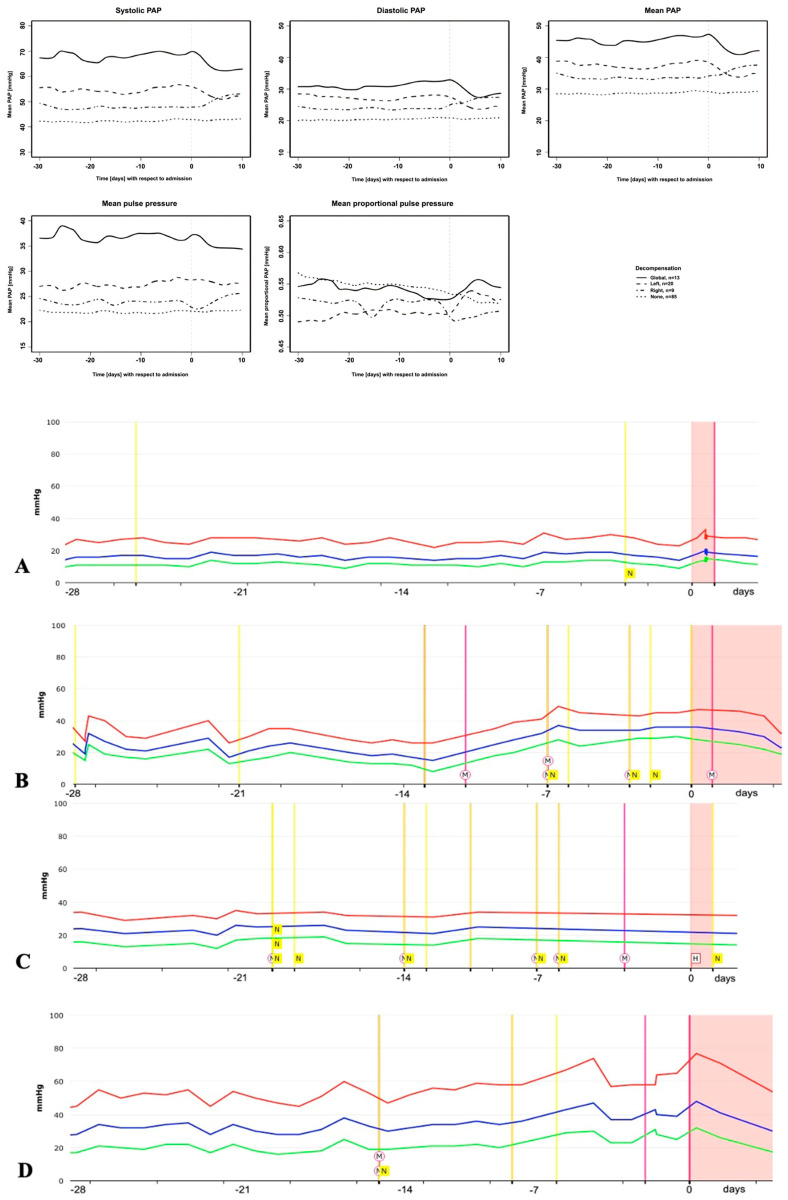
Background/Objectives: Patients with New York Heart Association (NYHA) class III heart failure (HF) suffer from frequent hospitalizations. Non-invasive pulmonary artery pressure (PAP) sensor-guided HF care has been shown to reduce hospitalizations. However, it is unknown whether the PAP changes prior to hospitalization differ between clinical right, left or global cardiac decompensation. Methods: Sensor-derived PAP data and HF hospitalization records from 41 patients with NYHA class III HF were classified retrospectively into predominantly left, right or global decompensation. Linear mixed-effect regression models were used for statistical evaluations of the PAP in selected hospitalizations for which admission was at least 28 days after the last admission and 14 days after the last hospital discharge and with readings in between. Results: During 24.4 months of follow-up, 127 hospitalizations in 38 patients were evaluated. The global cardiac decompensation (n = 13) had the highest PAP before hospitalization, followed by left-sided (n = 20) decompensation. Patients with right-sided decompensation (n = 9) had comparable PAP values before hospitalization to the cohort without any cardiac decompensation (n = 85). The diastolic PAP showed a significant increase of 0.035 mmHg/day (p = 0.0097) in left-sided decompensation and of 0.13 mmHg/day (p < 0.0001) in global cardiac decompensation, whereas no significant change in the diastolic PAP occurred prior to the right-sided decompensation. The baseline right ventricular function and right ventricle-pulmonary arterial coupling (TAPSE/PASP ratio) were impaired in patients with subsequent global cardiac decompensation. Conclusion: PAP telemonitoring-guided therapy can reliably detect early signs of left and global cardiac decompensation but may be limited in detecting right-sided cardiac congestion. The routine assessment of RV-PA coupling may improve the detection of global cardiac decompensation, as severe impairments could indicate impending deterioration. In contrast, monitoring the RV contractility may aid in identifying isolated right-sided congestion and imminent decompensation.
Keywords: chronic heart failure; pulmonary artery pressure; remote monitoring; right-sided decompensation.
Conflict of interest statement
BA reports having received consulting fees and an unrestricted research grant from St Jude Medical, which is now Abbott, and lecture fees from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Meyers Squibb, Edwards, Novartis, Pfizer and CSL Vifor. EJH reports receiving lecture fees from Bayer and CSL Vifor.
Figures
References
-
- Benjamin E.J., Muntner P., Alonso A., Bittencourt M.S., Callaway C.W., Carson A.P., Chamberlain A.M., Chang A.R., Cheng S., Das S.R., et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation. 2019;139:e56–e528. doi: 10.1161/CIR.0000000000000659. - DOI - PubMed
-
- Nieminen M.S., Brutsaert D., Dickstein K., Drexler H., Follath F., Harjola V.-P., Hochadel M., Komajda M., Lassus J., Lopez-Sendon J.L., et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006;27:2725–2736. doi: 10.1093/eurheartj/ehl193. - DOI - PubMed
-
- Russo M.J., Gelijns A.C., Stevenson L.W., Sampat B., Aaronson K.D., Renlund D.G., Ascheim D.D., Hong K.N., Oz M.C., Moskowitz A.J., et al. The Cost of Medical Management in Advanced Heart Failure During the Final Two Years of Life. J. Card. Fail. 2008;14:651–658. doi: 10.1016/j.cardfail.2008.06.005. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
