

Pituitary Apoplexy in a Child with Short Stature and Possible Recent SARS-CoV-2 Infection
- PMID: 40564774
- PMCID: PMC12192251
- DOI: 10.3390/diagnostics15121453
Pituitary Apoplexy in a Child with Short Stature and Possible Recent SARS-CoV-2 Infection
Abstract
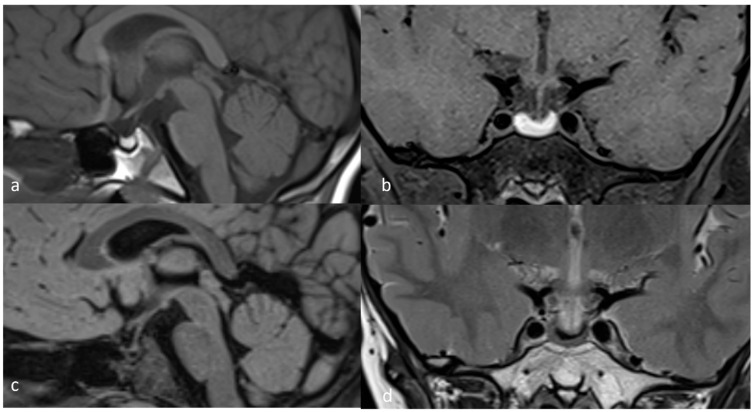
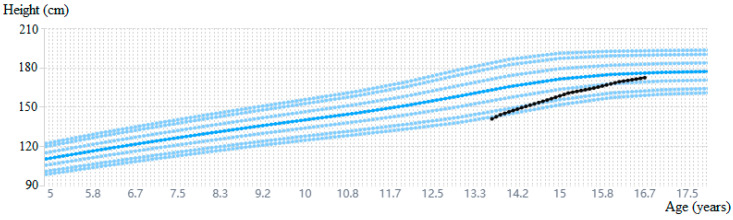
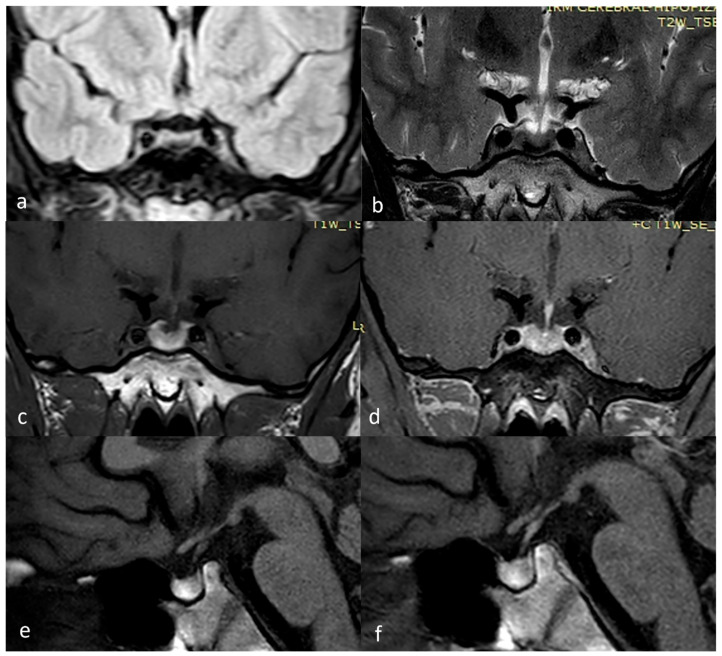
Background and Clinical Significance: Pituitary apoplexy is an extremely rare condition in children and adolescents with a rapid onset due to acute hemorrhage, infarction, or both in the pituitary gland. Most frequently, pituitary apoplexy is an asymptomatic or subclinical entity. Few cases of pituitary apoplexy with concurrent SARS-CoV-2 infection or COVID-19 vaccination have been reported. Case Presentation: We present the case of a 13-year-8-month-old boy who presented in our pediatric endocrinology department for the evaluation of short stature. He was previously diagnosed with secondary hypothyroidism and was treated with levothyroxine. At admission, clinical examination revealed a height of 141 cm (-2.68 SD/-2.4 SD corrected for mid-parental height), normal weight (60th centile), Tanner-stage G2P1, and delayed bone age. Basal IGF1 was normal, but the tests performed to assess the GH reserve confirmed the GH deficiency (peak GH value 3.11 ng/mL after clonidine/0.95 ng/mL after insulin). The brain MRI revealed a subacute pituitary hemorrhage. Thrombophilia and coagulopathies were excluded by further testing. Anti-SARS-CoV-2 (anti-S-protein IgG) antibodies (>200 BAU/mL) were compatible with COVID-19 infection, indicating a possible association between these two entities. At 3-month follow-up, physical examination showed a 3 cm height gain and advancing pubertal development (G4P2). Newer MRI found changes consistent with resolving hemorrhage. The patient was provided immediately with recombinant human GH and aromatase inhibitor therapy to maximize GH treatment response. During follow-up, the rGH dose was adjusted based on IGF1 values, and after 3 years and 10 months, rGH treatment was stopped, reaching a height of 172.3 cm (-0.51 SD) and surpassing the initial prediction of 164.5 cm. Conclusions: Pituitary apoplexy, an even rarer complication in the pediatric population, may be associated with SARS-CoV-2 infection. Further studies are necessary to better understand the intertwining of those conditions.
Keywords: COVID-19; aromatase inhibitor therapy; pituitary apoplexy; short stature.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Bonicki W., Kasperlik-Załuska A., Koszewski W., Zgliczyński W., Wisławski J. Pituitary Apoplexy: Endocrine, Surgical and Oncological Emergency. Incidence, Clinical Course and Treatment with Reference to 799 Cases of Pituitary Adenomas. Acta Neurochir. 1993;120:118–122. doi: 10.1007/BF02112028. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
