

Pessary for Prevention of Preterm Birth and Perinatal Mortality in Pregnancies with a Short Cervix: Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 40564787
- PMCID: PMC12191806
- DOI: 10.3390/diagnostics15121466
Pessary for Prevention of Preterm Birth and Perinatal Mortality in Pregnancies with a Short Cervix: Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
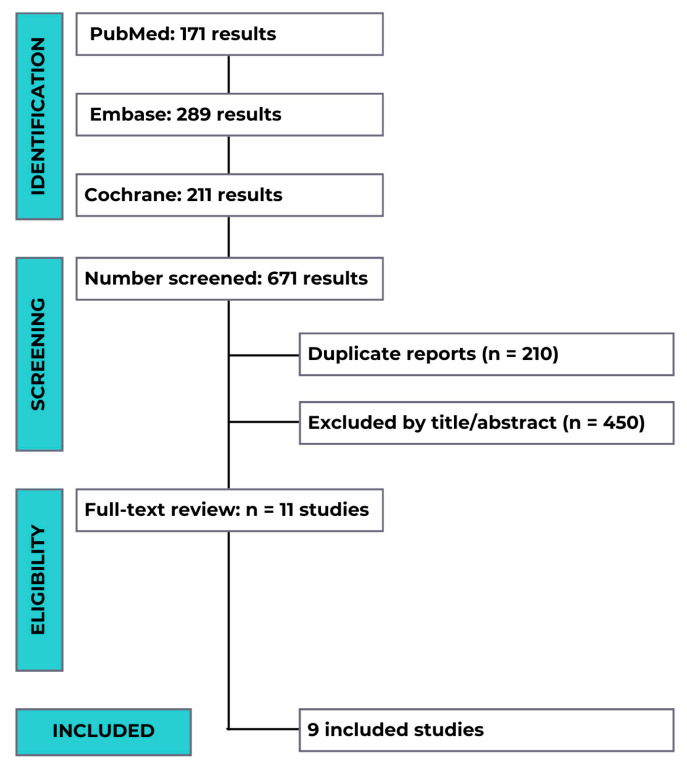
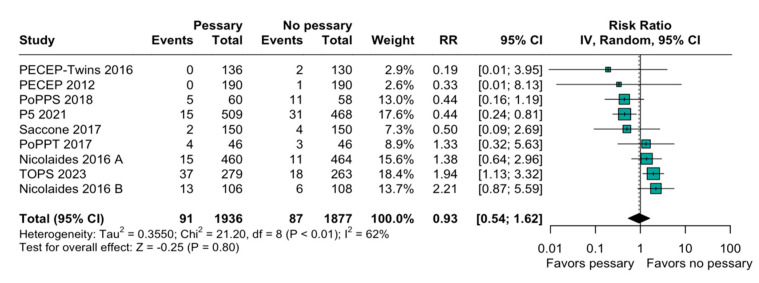
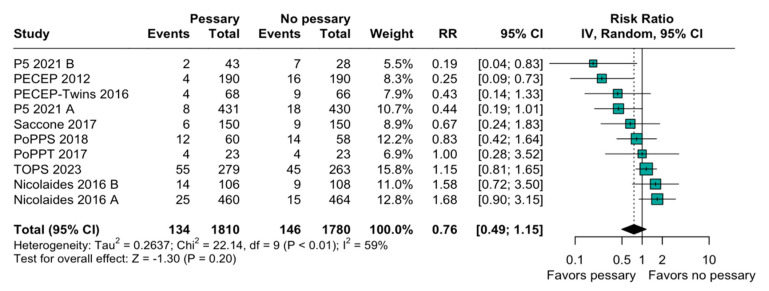
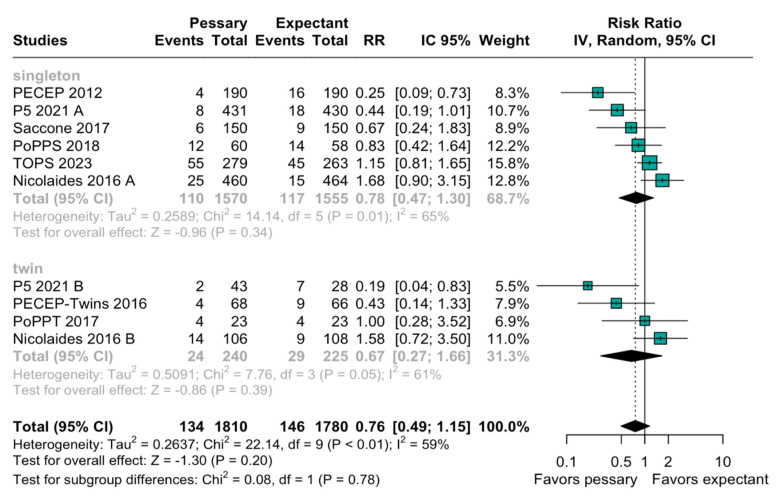
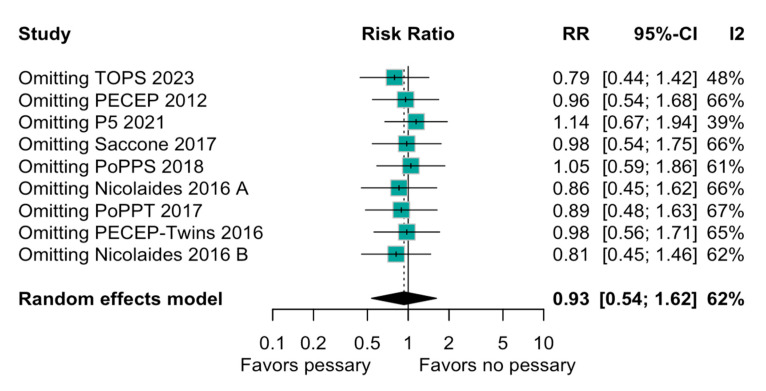
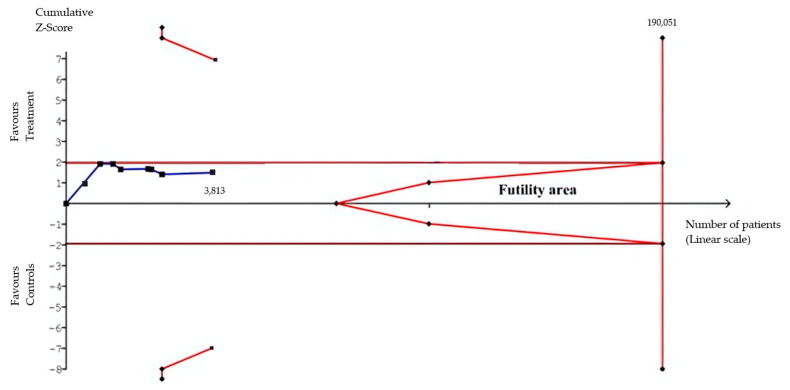
Objective: This systematic review and meta-analysis aimed to evaluate the efficacy of cervical pessaries in preventing perinatal mortality and extreme preterm birth in pregnancies characterized by a short cervix. Methods: The analysis included data from nine randomized controlled trials (RCTs), incorporating a total of 3813 participants. These studies compared the use of cervical pessaries against standard care or other interventions in preventing preterm births in women with a short cervix, defined as less than 30 mm. The eligibility criteria for the trials included studies on asymptomatic pregnant women with a short cervix. The primary outcomes analyzed were perinatal mortality and the incidence of preterm birth before 28 weeks of gestation. Results: The results showed an imprecise effect estimate for perinatal mortality (OR = 0.93; 95% CI: 0.54 to 1.62). Similarly, the risk reduction for preterm birth before 28 weeks was also non-significant (OR = 0.76; 95% CI: 0.49 to 1.15). Substantial heterogeneity was observed among the studies (I2 = 62%), suggesting variability in the study results, which could have been influenced by differences in the study design, population, and interventions. Conclusions: Although the results were statistically inconclusive and the estimates imprecise, the confidence intervals still span possible benefit and harm. Thus, while the current evidence does not support the routine use of cervical pessaries, it also does not indicate an increased risk of fetal or neonatal mortality.
Keywords: cervical pessary; perinatal mortality; preterm birth; short cervix; systematic review.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Liu L., Oza S., Hogan D., Perin J., Rudan I., Lawn J.E., Cousens S., Mathers C., Black R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet. 2015;385:430–440. doi: 10.1016/S0140-6736(14)61698-6. - DOI - PubMed
-
- França M.S., Hatanaka A.R., Cruz J.D.J., Júnior L.D.A., Emy T., Hamamoto K., Sarmento S.G.P., Júnior J.E., Pares D.B.d.S., Mattar R., et al. Cervical pessary plus vaginal progesterone in a singleton pregnancy with a short cervix: An experience-based analysis of cervical pessary’s efficacy. J. Matern.-Fetal Neonatal Med. 2021;35:6670–6680. doi: 10.1080/14767058.2021.1919076. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
