

The Hôtel-Dieu MRI Classification of Uterosacral Ligament Involvement in Endometriosis: A Pictorial Guide to Clinical Use
- PMID: 40564829
- PMCID: PMC12192483
- DOI: 10.3390/diagnostics15121508
The Hôtel-Dieu MRI Classification of Uterosacral Ligament Involvement in Endometriosis: A Pictorial Guide to Clinical Use
Abstract
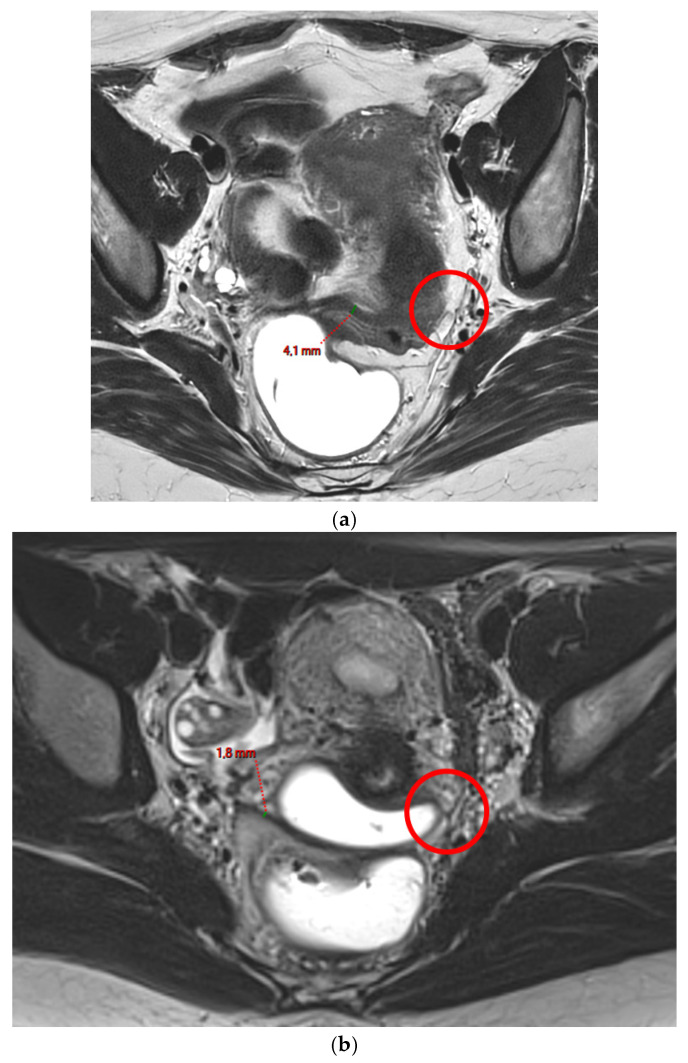
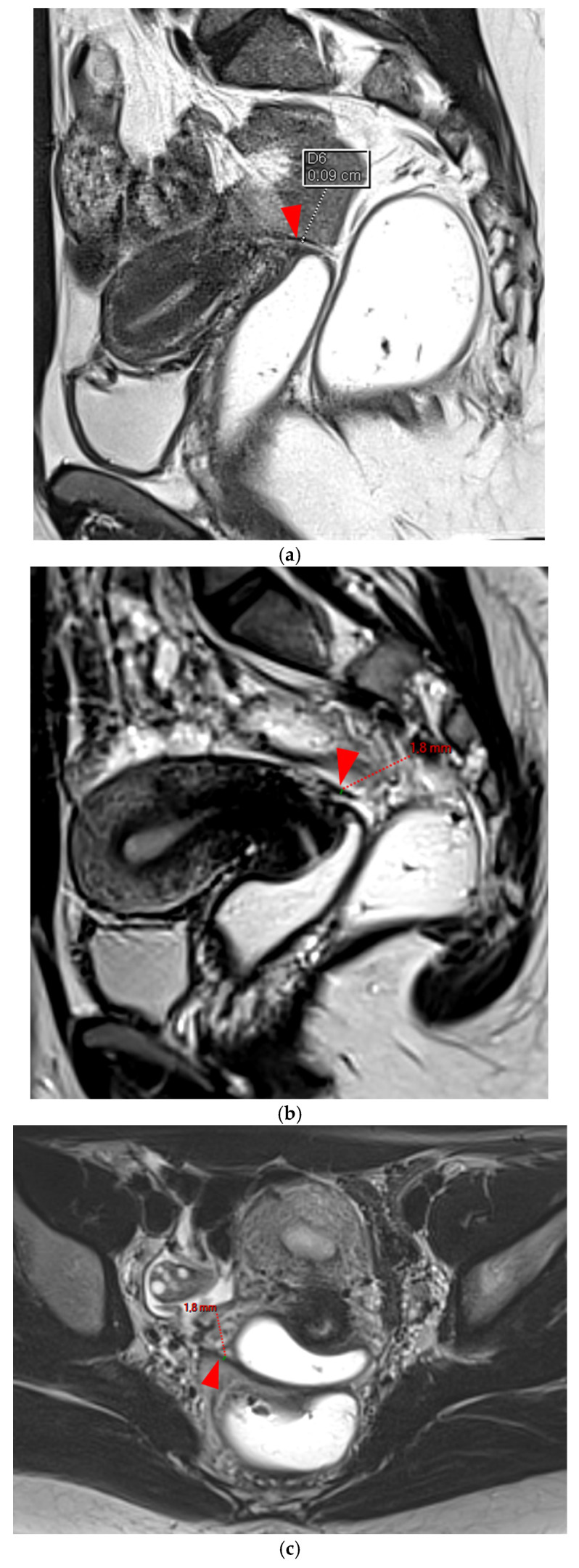
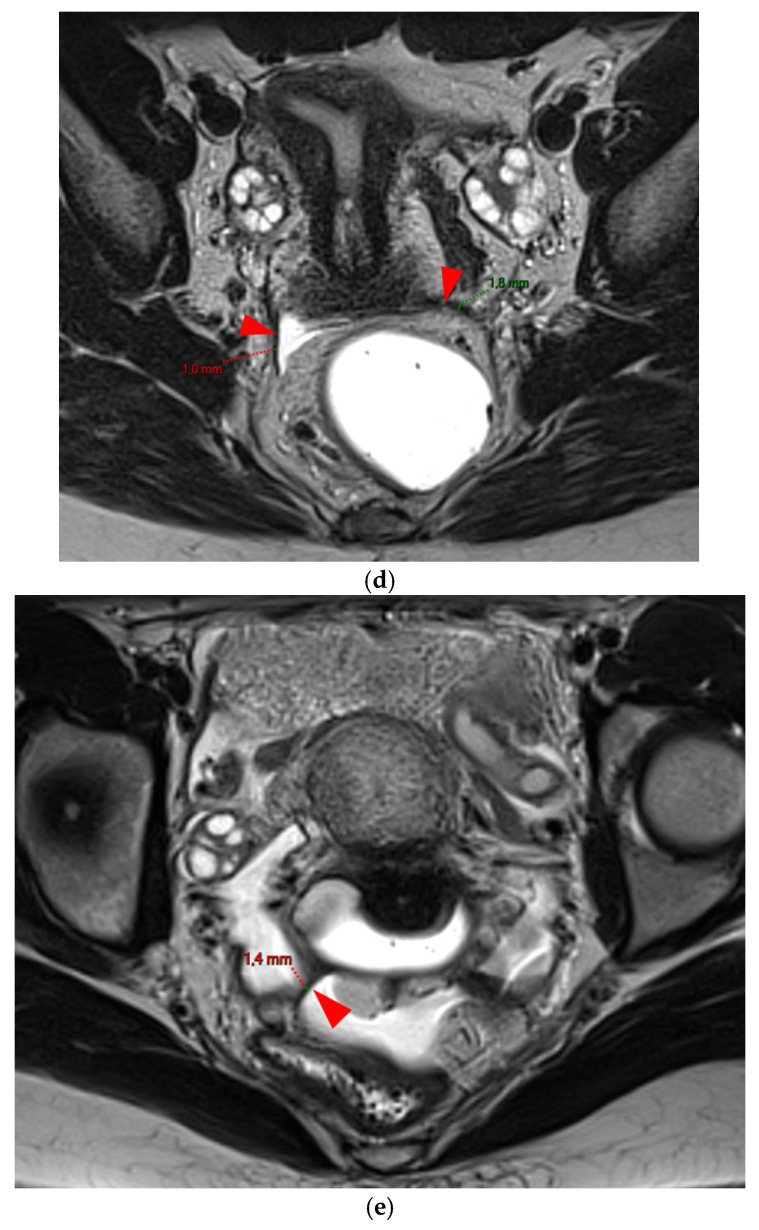
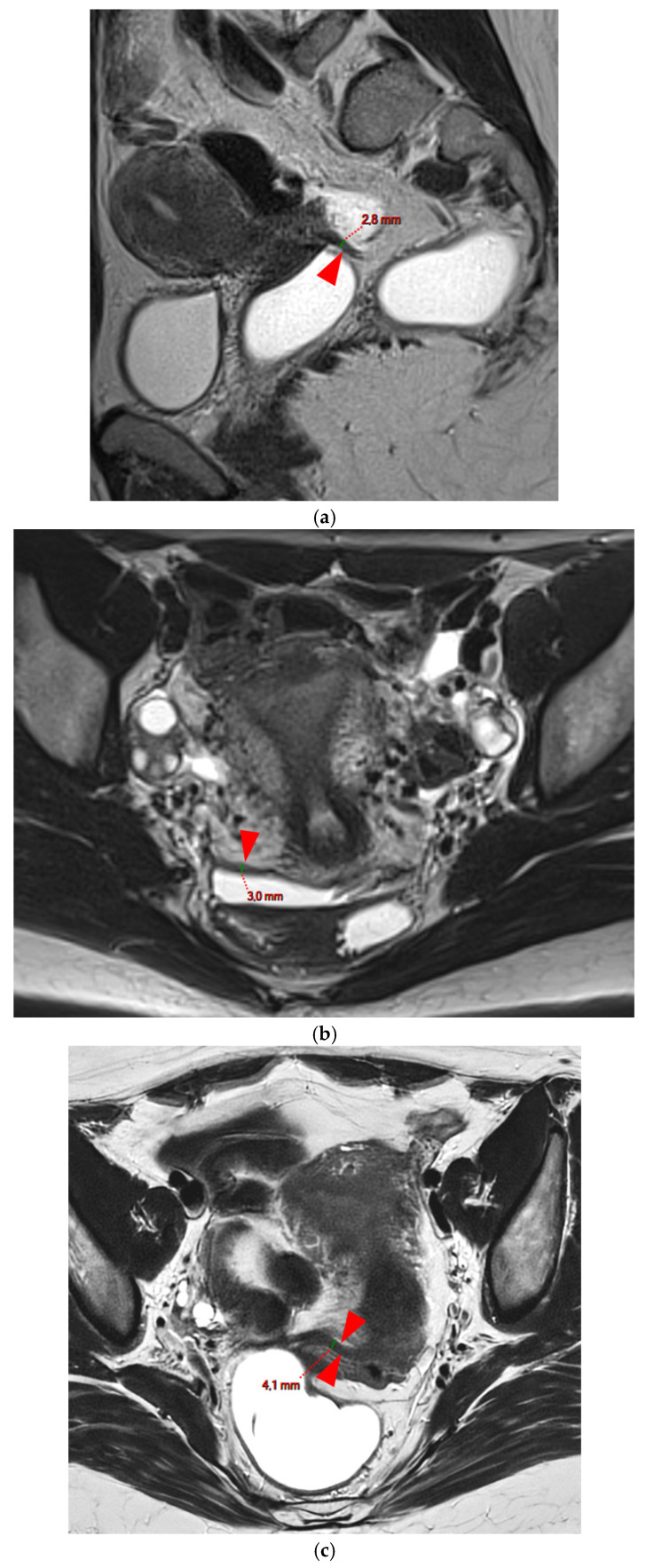
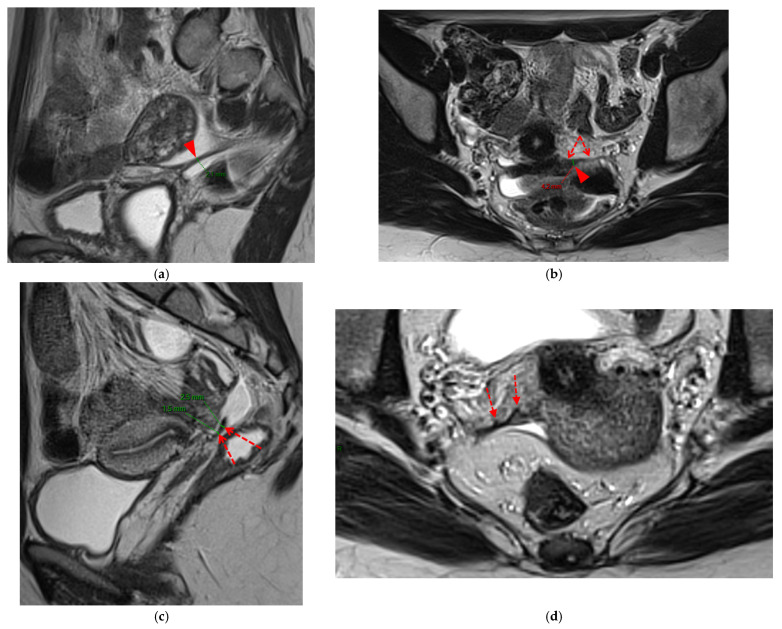
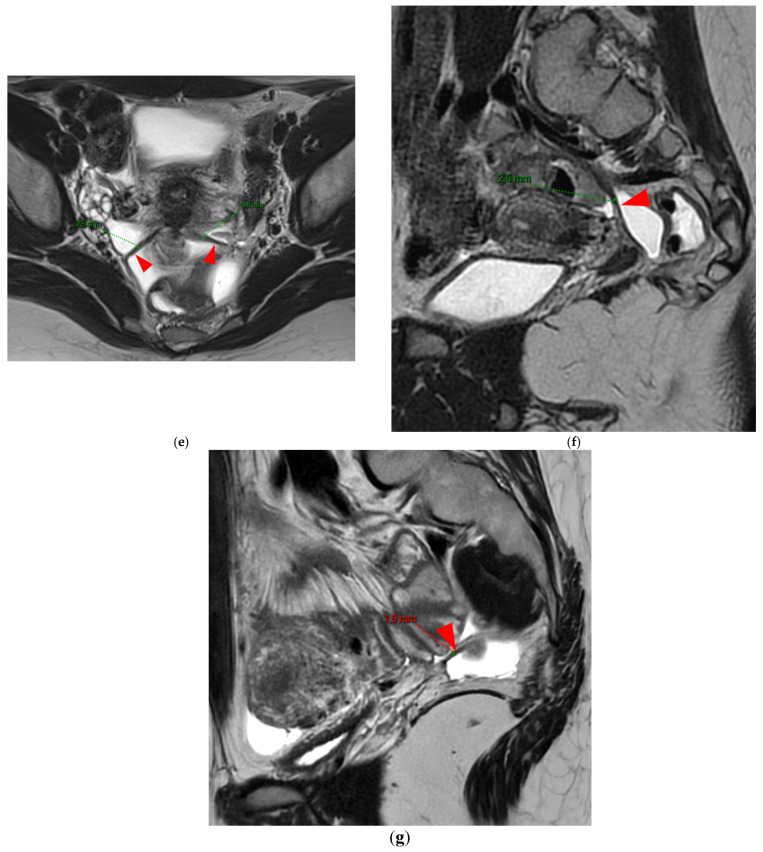
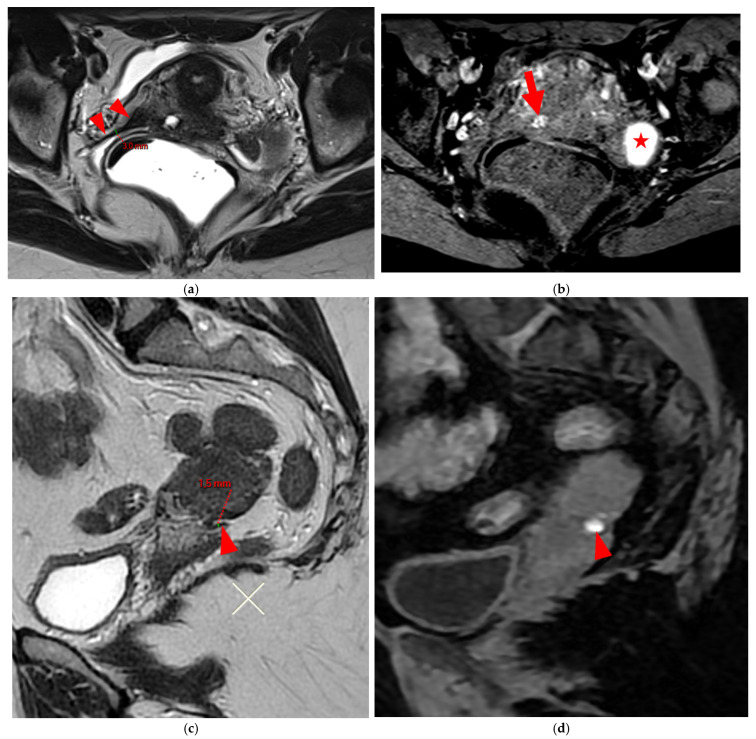
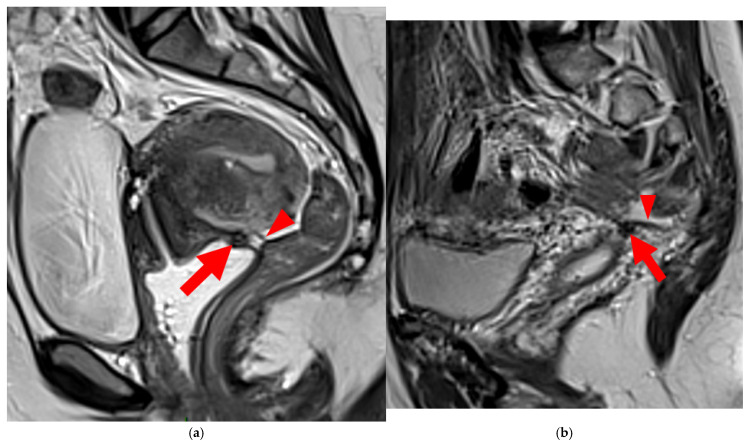
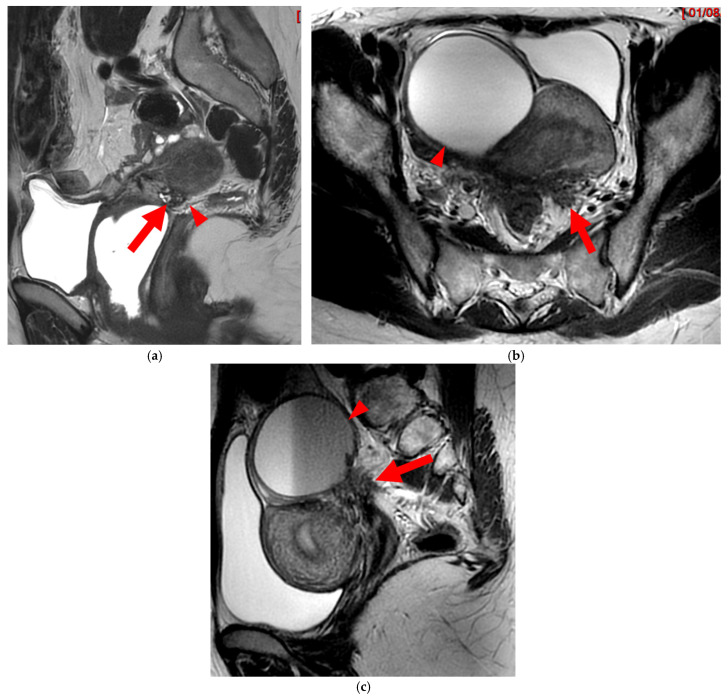
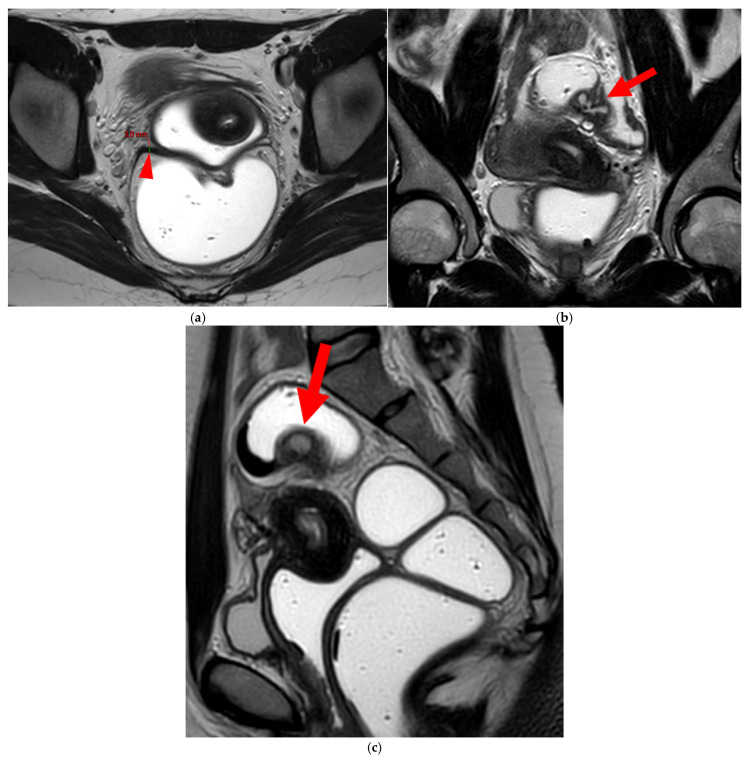
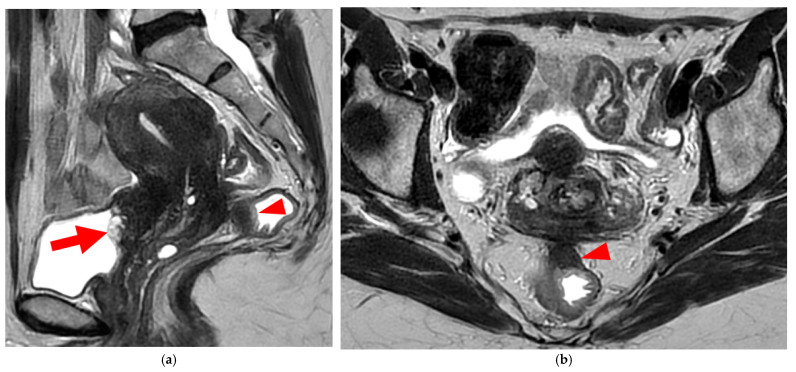
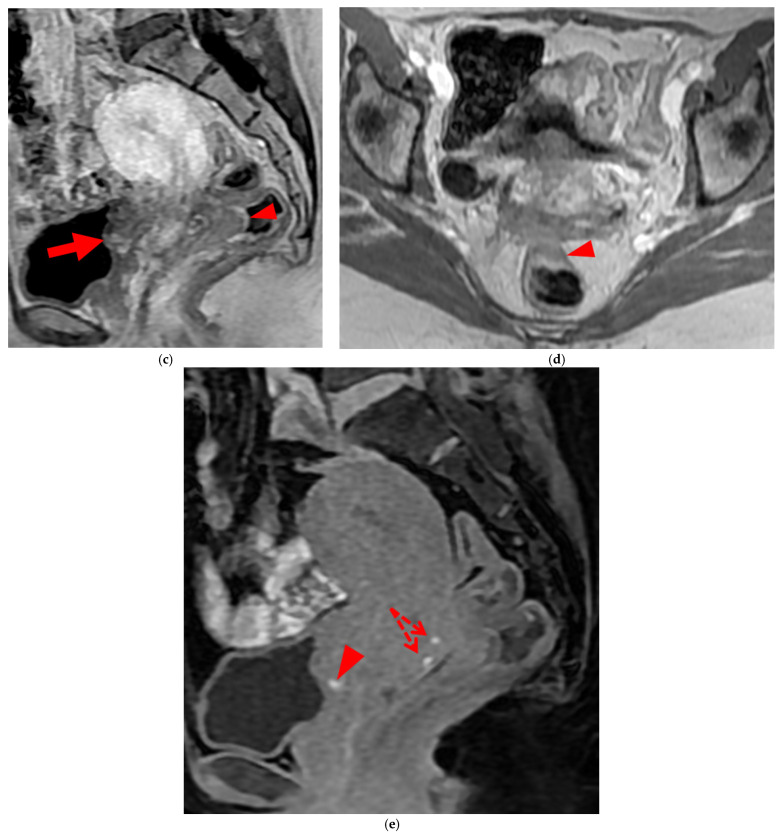
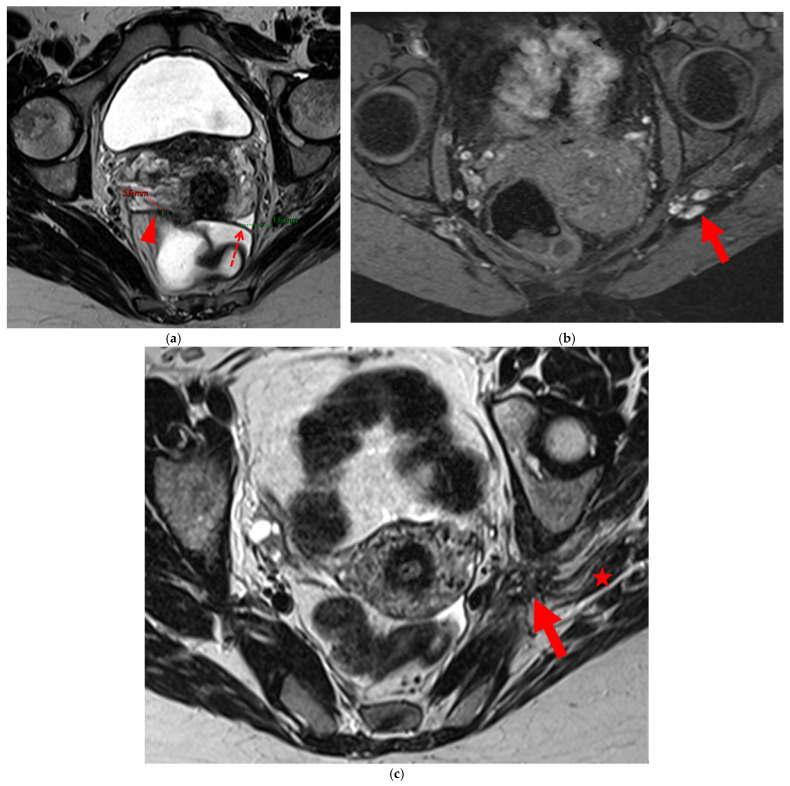
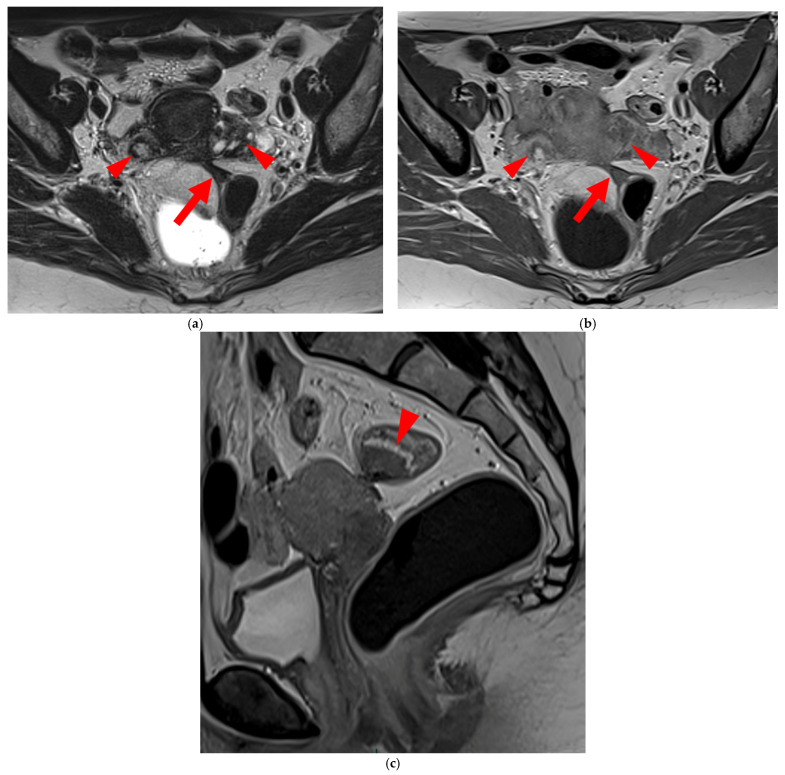
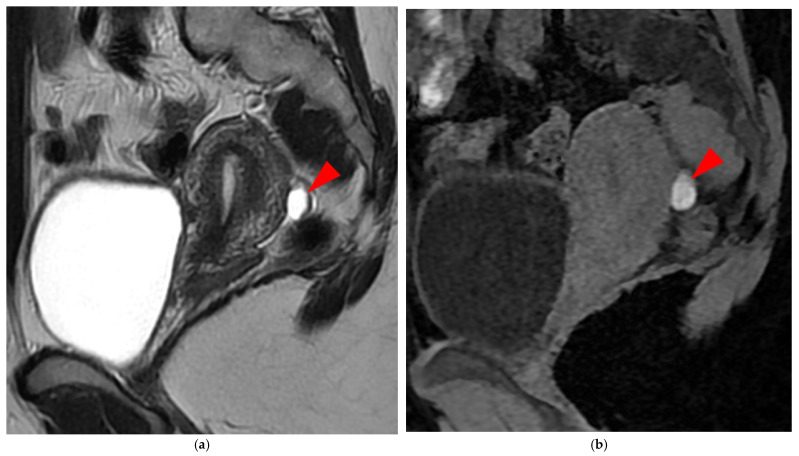
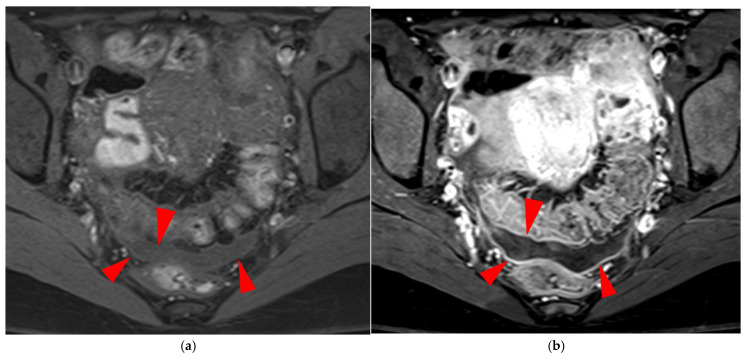
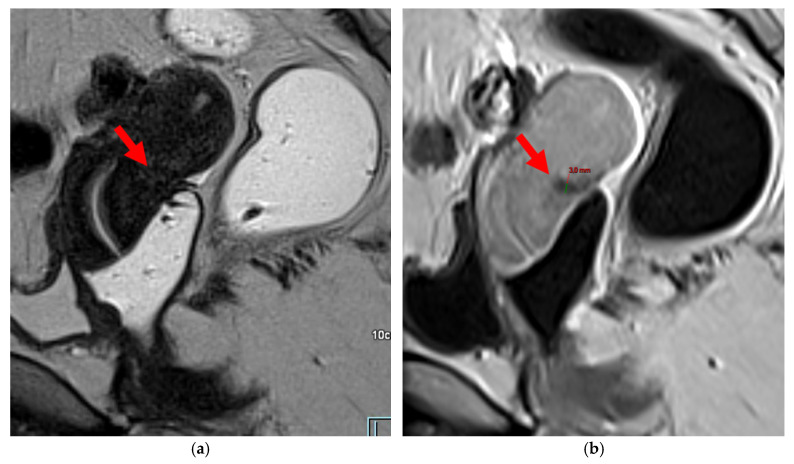
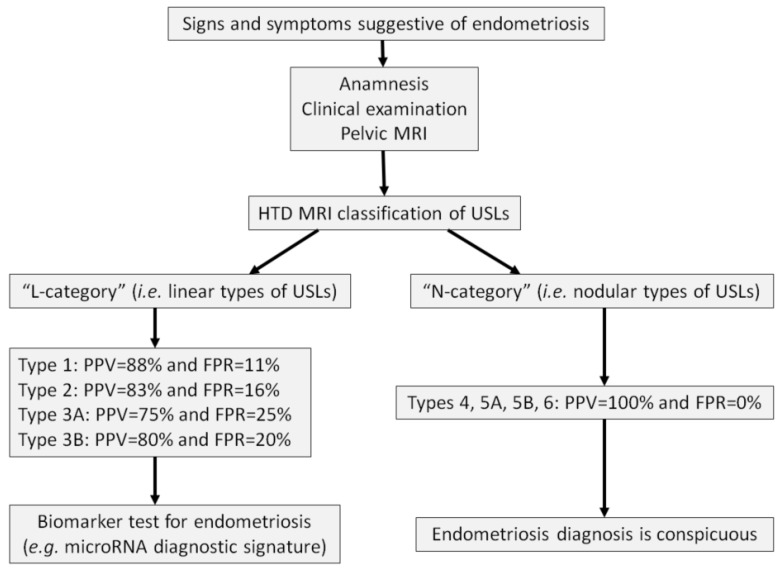
Objectives: Endometriosis is a common gynecologic condition characterized by the presence of endometrial-like tissue outside the uterus, often leading to pelvic pain and infertility. Diagnosis is frequently delayed, with prolonged diagnostic wandering that could be improved through enhanced first-line radiologic assessment. The uterosacral ligament (USL) is the most frequent site of deep infiltrating endometriosis (DIE). The Hôtel-Dieu (HTD) MRI classification, published in 2024, offers a structured framework for evaluating USL involvement by correlating MRI findings with the diagnostic certainty of endometriosis. Key Findings: This pictorial essay provides a practical guide for applying the HTD MRI classification, presenting key imaging criteria with illustrative examples for each USL type. The classification distinguishes between "linear" and "nodular" USL lesions, with implications for diagnostic confidence. "Nodular" types demonstrate a 100% positive predictive value (PPV), while "linear" types may yield higher false positive rates (FPR). The HTD MRI classification may also be complemented by innovative biomarker testing, such as microRNA signatures, especially in cases with "linear" USL involvement. Conclusions: By standardizing the assessment of USL lesions, the HTD MRI classification enhances diagnostic accuracy, improves MRI reproducibility, and supports earlier identification of endometriosis in first-line settings. Its integration into radiologic workflows can contribute to reduced diagnostic delays. Implications for practice: The HTD MRI classification is a valuable screening tool for first-line radiologists and clinicians. Incorporating it into routine pelvic MRI interpretations may streamline diagnostic pathways, promote consistency across readers, and guide additional testing strategies, such as microRNA assays, for cases where MRI alone is less definitive.
Keywords: DIE; HTD; Hôtel-Dieu; MRI classification; USL; deep infiltrating endometriosis; miRNA; microRNA; uterosacral ligament.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Clement M.D. Diseases of the peritoneum (including endometriosis) In: Kurman R.J., editor. Blaustein’s Pathology of the Female Genital Tract. Volume 1 Springer; New York, NY, USA: 2002.
Publication types
LinkOut - more resources
Full Text Sources
