

Early Cardiovascular and Metabolic Benefits of rhGH Therapy in Adult Patients with Severe Growth Hormone Deficiency: Impact on Oxidative Stress Parameters
- PMID: 40564898
- PMCID: PMC12192984
- DOI: 10.3390/ijms26125434
Early Cardiovascular and Metabolic Benefits of rhGH Therapy in Adult Patients with Severe Growth Hormone Deficiency: Impact on Oxidative Stress Parameters
Abstract
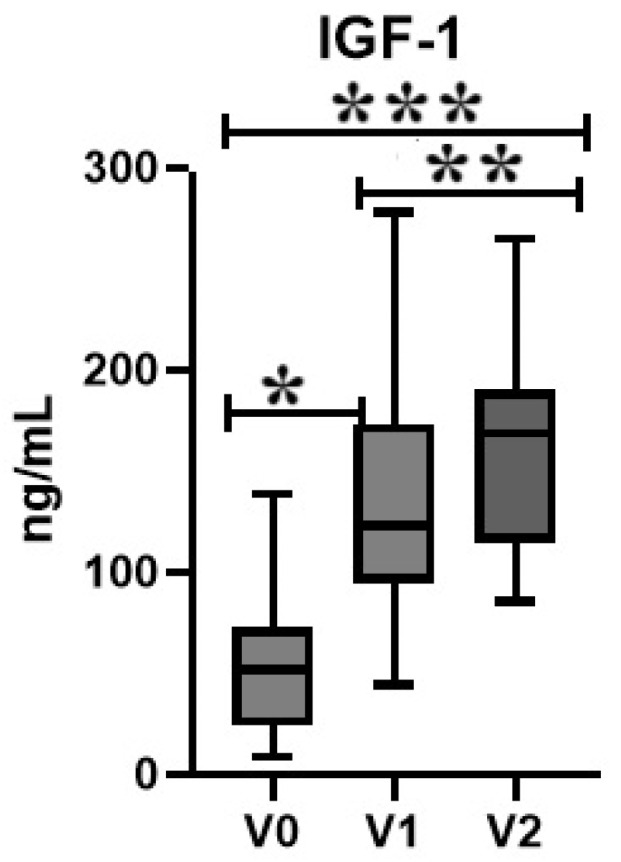
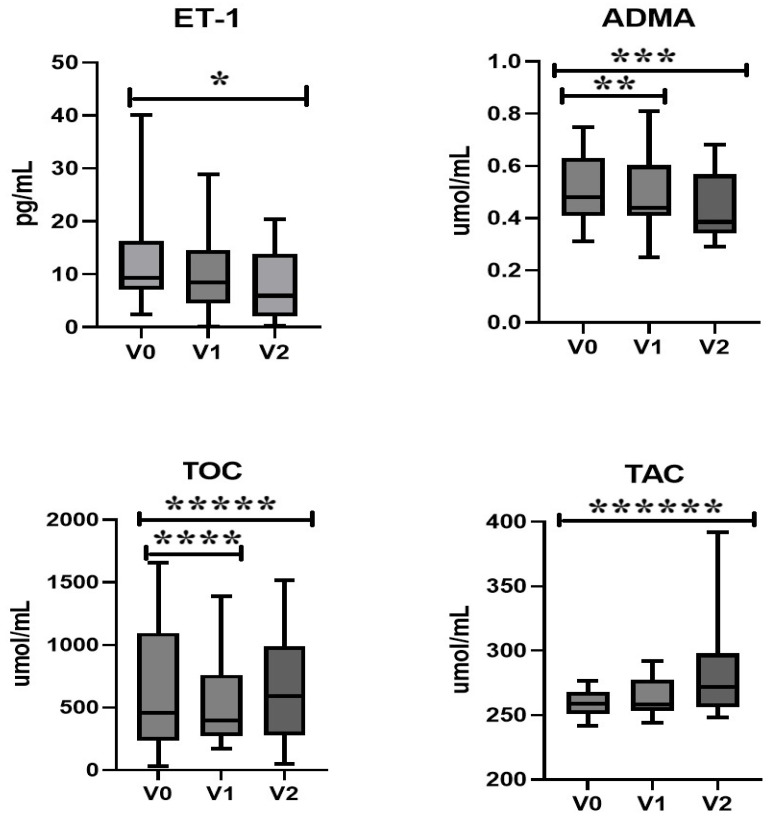
It is hypothesized that growth hormone deficiency (GHD) is associated with increased oxidative stress (OS), contributing to elevated cardiovascular risk. This preliminary study evaluates changes in OS markers and cardiovascular biomarkers in 15 adult patients with severe GHD undergoing 12 months of recombinant human growth hormone (rhGH) therapy. IGF-1 concentrations increased significantly following 6 and 12 months of therapy (p = 0.0003 and p = 0.0001, respectively). These changes were accompanied by a significant decrease in endothelin-1 (ET-1) levels at 12 months (p = 0.007), as well as reductions in asymmetric dimethylarginine (ADMA) levels at both 6 and 12 months (p = 0.01 for each timepoint). Total oxidative capacity (TOC) decreased significantly after 6 months of therapy (p = 0.02), followed by a significant increase at 12 months (p = 0.04), whereas total antioxidant capacity (TAC) showed a significant increase at 12 months (p = 0.02). Tissue fat % showed significant reductions at 6 months (p = 0.006), suggesting early improvements in body composition. Correlation analyses indicated negative associations between IGF-1 and TOC (p < 0.006; R = -0.73), and positive associations with TAC (p < 0.001; R = 0.83). These findings suggest that rhGH therapy in adult patients with severe GHD reduces OS and cardiovascular risk through the modulation of biomarkers and improved body composition. This study explores the role of rhGH therapy in reducing cardiovascular risks in GHD, emphasizing the importance of individualized treatment approaches.
Keywords: asymmetric dimethyl arginine; endothelin-1; growth hormone; growth hormone deficiency; oxidative stress.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Collett-Solberg P.F., Ambler G., Backeljauw P.F., Bidlingmaier M., Biller B.M., Boguszewski M.C., Cheung P.T., Choong C.S.Y., Cohen L.E., Cohen P., et al. Diagnosis, Genetics, and Therapy of Short Stature in Children: A Growth Hormone Research Society International Perspective. Horm. Res. Paediatr. 2019;92:1–14. doi: 10.1159/000502231. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
