

A Systematic Review and Meta-Analysis on the Efficacy and Safety of Concomitant Laparoscopic Cholecystectomy and Sleeve Gastrectomy in Patients with Morbid Obesity
- PMID: 40565853
- PMCID: PMC12194429
- DOI: 10.3390/jcm14124108
A Systematic Review and Meta-Analysis on the Efficacy and Safety of Concomitant Laparoscopic Cholecystectomy and Sleeve Gastrectomy in Patients with Morbid Obesity
Abstract
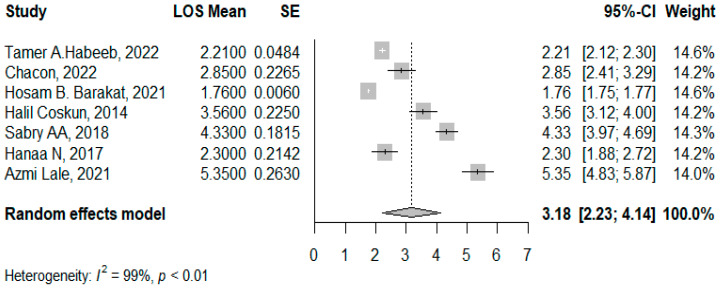
Background/Objectives: Rapid weight loss after bariatric surgery is linked to a higher risk of symptomatic gallstone disease, which could require a cholecystectomy. This meta-analysis aimed to assess the efficacy and safety of conducting laparoscopic cholecystectomy concurrently with sleeve gastrectomy in morbid obese patients. Methods: Scopus, PubMed, ProQuest, Web of Science, and Google Scholar were searched for this review. Quality assessment was conducted using the Newcastle-Ottawa Scale for observational studies and ROB2 for randomized clinical trials. Eight of thirteen studies were high-quality. Pooling for BMI difference and LOS was used to measure efficacy, and the pooled proportion was utilized to assess safety through bleeding, wound infection, and leakage. Heterogeneity was explained via leave-one-out analysis and meta-regression. Results: The pooled standardized mean difference in BMI peri-operation was 3.26 (95% CI: 2.51-4.01, p < 0.01), where the age and initial BMI explained 98% of the heterogeneity through meta-regression. The pooled mean of LOS was 3.18 days (95% CI: 2.23-4.14, I2 = 99%, p < 0.001), where age explained 33.22% of the heterogeneity through meta-regression. The pooled proportion of bleeding was 0.03 (95% CI: 0.02-0.04, I2 = 2%, p = 0.42). The pooled wound infection was 0.04 (95% CI: 0.02-0.08, I2 = 80%, p < 0.001), where age accounted for 99% of the heterogeneity. The pooled biliary/gastric leakage was 0.02 (95% CI: 0.01-0.05, I2 = 0, p = 0.52). Conclusions: These findings indicate that the combined procedures can be executed with an acceptable safety profile. The heterogeneity in outcomes underscores the necessity of personalized patient care, standardized perioperative practices, and continuous research to enhance results and mitigate dangers.
Keywords: complications; efficacy; laparoscopic cholecystectomy (LC); morbid obesity; sleeve gastrectomy (SG); weight loss.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures










References
-
- Abo-Ryia M.H., Abd-Allah H.S., El-Khadrawy O.H., Moussa G.I. Predictors of gallstone formation in morbidly obese patients after bariatric surgery: A retrospective observational study. Surg. Sci. 2014;5:1–5. doi: 10.4236/ss.2014.51001. - DOI
-
- Sattaratnamai A., Samankatiwat N., Udomsawaengsup S., Ratchaburi Hospital. King Chulalongkorn Memorial Hospital . Subsequent Cholecystectomy Rate After Bariatric Surgery in Morbid Obesity Patients: A Systematic Review and Meta-Analysis. SAGE; Newcastle upon Tyne, UK: 2015.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
