

Ureteric Complications and Urinary Tract Reconstruction Techniques in Renal Transplantation: A Surgical Essay
- PMID: 40565879
- PMCID: PMC12193927
- DOI: 10.3390/jcm14124129
Ureteric Complications and Urinary Tract Reconstruction Techniques in Renal Transplantation: A Surgical Essay
Abstract
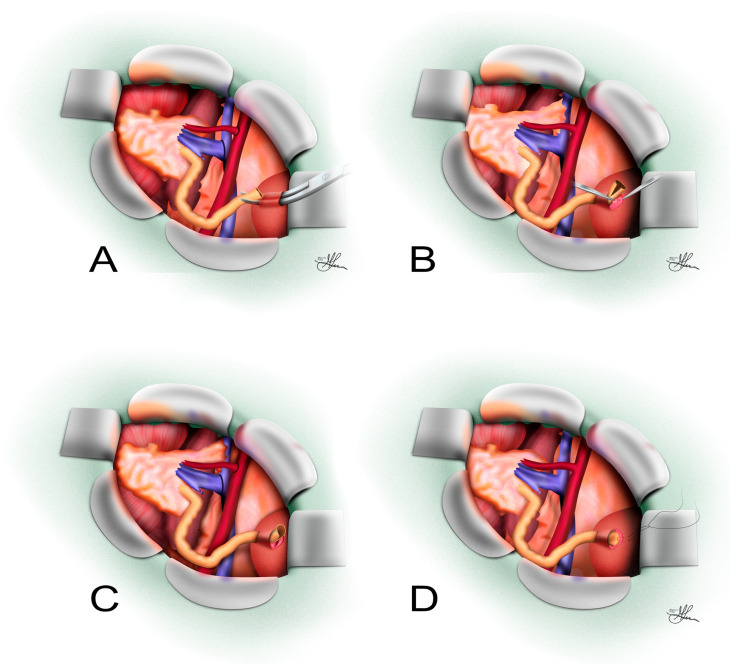
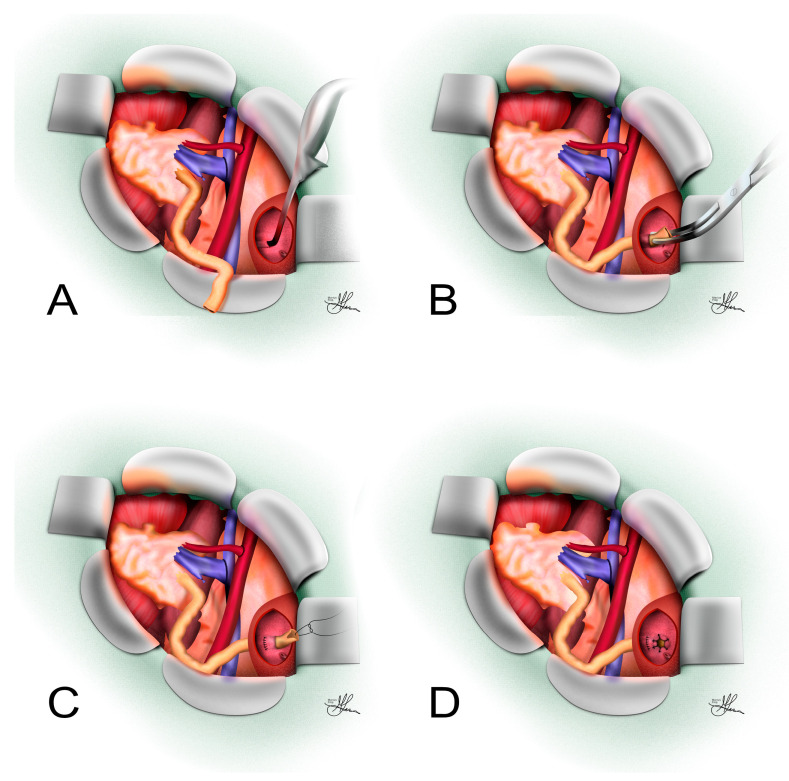
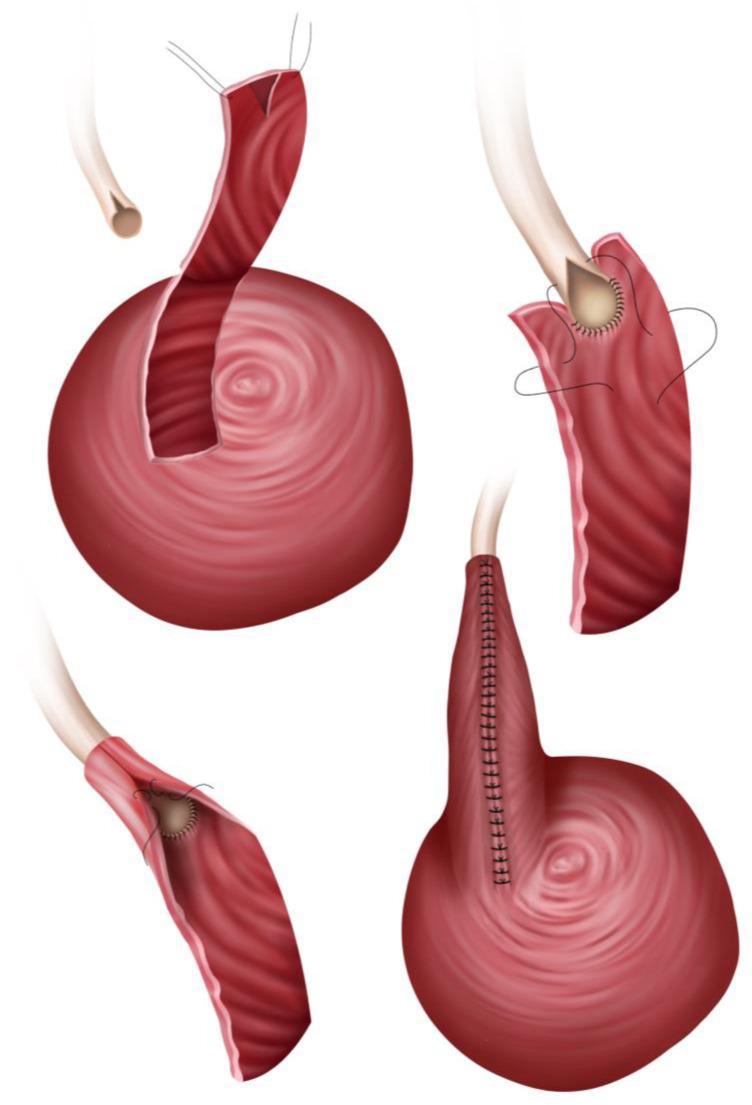
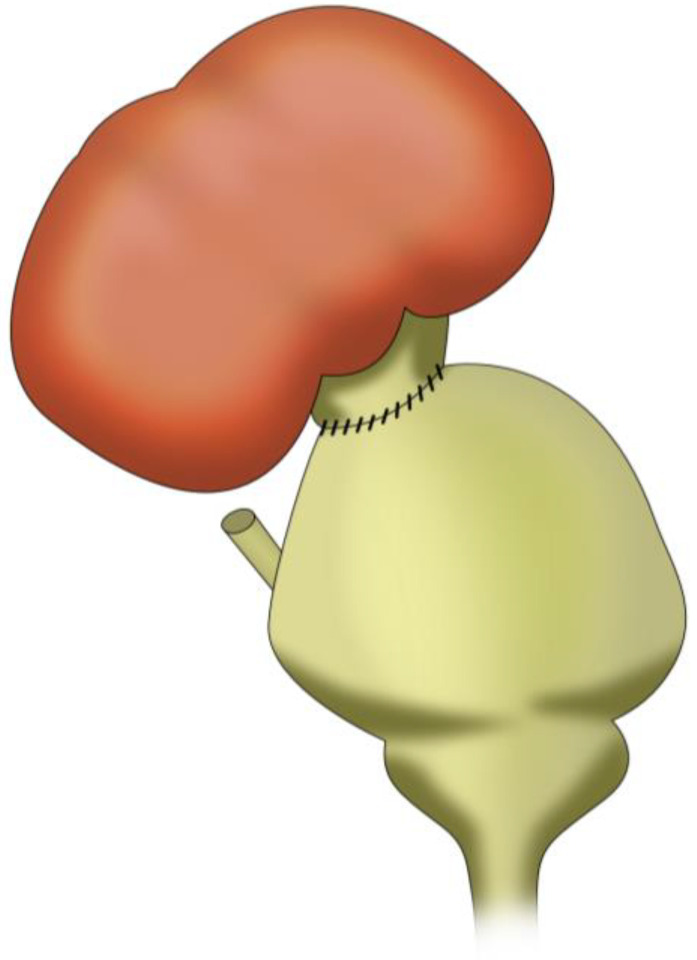
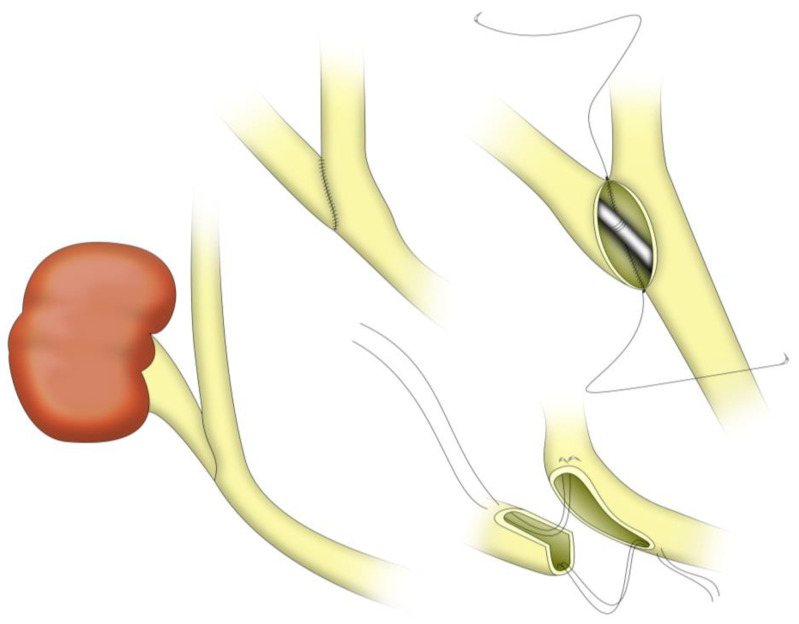
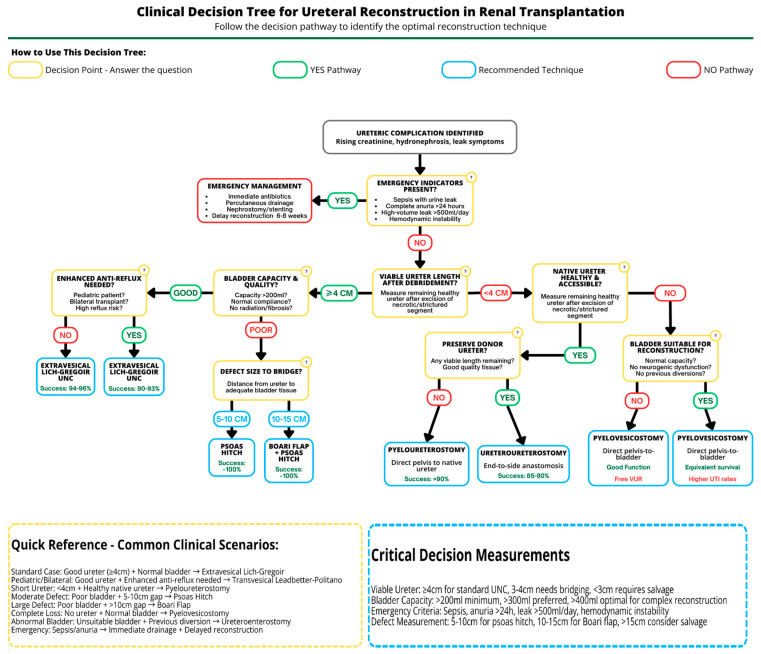
Background/Objectives: Renal transplantation (RT) remains the gold standard for end-stage renal disease, offering superior outcomes versus dialysis. Despite advances, ureteric complications (leaks/strictures) persist, primarily from ischemic injury, posing substantial graft risks. We review etiology, incidence, and management strategies for post-RT ureteric complications, focusing on surgical reconstruction techniques. Methods: Literature assessment examined ischemic-related ureteric complications. Primary outcomes: incidence, success, complication rates, operative times, and long-term patency. Secondary outcomes: graft/patient survival and reoperation rates. Techniques evaluated included extravesical Lich-Gregoir (L-G) and transvesical Leadbetter-Politano (L-P) ureteroneocystostomy (UNC), Boari flap with psoas hitch, pyelo/ureteroureterostomy, pyelovesicostomy, and ureteroenterostomy. Surgical indications, procedural details, advantages, disadvantages, and quantitative outcomes were systematically analyzed. Results: Ureteric complication incidence ranged from 1 to 15%, with ischemic injury as the primary cause. L-G UNC demonstrated lower complication rates than L-P (6.15% vs. 8.33%) with reduced operative times. Pyelo/ureteroureterostomy achieved excellent salvage outcomes (>90% success, 3.9% reintervention rate). Boari flap provides a suitable option for extensive ureteric defects, consistently preserving graft function without stricture recurrences. Pyelovesicostomy showed 80% long-term success in complex cases. Ureteroenterostomy achieved comparable 5-year graft survival (63%) to standard drainage, despite higher infection rates (65%). Pyelovesicostomy and ureteroenterostomy remain important solutions for specific challenging scenarios. Conclusions: Urinary reconstruction technique selection should be individualized based on anatomical considerations, pathology, and surgical expertise. Comprehensive understanding of reconstruction techniques enables effective management of ureteric complications, preserving graft function and improving outcomes.
Keywords: kidney transplantation; long-term outcomes; native upper tract anastomosis; post-transplant care; pyeloureterostomy and ureteroureterostomy; strictures and urinary leaks; surgical challenges in urinary reconstruction; ureteric complications; ureteroenterostomy; ureteroneocystostomy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Comparison of Urologic Complications Between Ureteroneocystostomy and Ureteroureterostomy in Renal Transplant: A Meta-Analysis.Exp Clin Transplant. 2016 Jun;14(3):276-81. doi: 10.6002/ect.2015.0161. Epub 2016 Feb 26. Exp Clin Transplant. 2016. PMID: 26925612
-
Early versus late ureteric stent removal after kidney transplantation.Cochrane Database Syst Rev. 2018 Jan 29;1(1):CD011455. doi: 10.1002/14651858.CD011455.pub2. Cochrane Database Syst Rev. 2018. PMID: 29376218 Free PMC article.
-
Surgical approach to hysterectomy for benign gynaecological disease.Cochrane Database Syst Rev. 2023 Aug 29;8(8):CD003677. doi: 10.1002/14651858.CD003677.pub6. Cochrane Database Syst Rev. 2023. PMID: 37642285 Free PMC article.
-
Medical and surgical interventions for the treatment of urinary stones in children.Cochrane Database Syst Rev. 2018 Jun 2;6(6):CD010784. doi: 10.1002/14651858.CD010784.pub2. Cochrane Database Syst Rev. 2018. PMID: 29859007 Free PMC article.
References
-
- Kusuma Duarsa G.W., Gede Oka A.A., Santosa K.B., Yudiana I.W., Wisnu Tirtayasa P.M., Putra Pramana I.B., Kloping Y.P. Successful Boari Flap Ureteroneocystostomy for Distal Ureteral Necrosis after Renal Transplantation. Urol. Case Rep. 2018;23:48–49. doi: 10.1016/j.eucr.2018.12.004. - DOI - PMC - PubMed
-
- Ogawa Y., Kono Y., Yagi Y., Ishizaka K., Suzuki H. Posttransplant Urine Leakage with Extensive Ureteral Stricture Corrected by Pyelopyelostomy: A Challenging Case. JOJ Urol. Nephrol. 2019;6:555690. doi: 10.19080/JOJUN.2019.06.555690. - DOI
-
- Harza M., Baston C., Preda A., Olaru V., Ismail G., Domnisor L., Daia D., Mitroi I., Baston M.O., Sinescu I. Impact of Ureteral Stenting on Urological Complications after Kidney Transplantation Surgery: A Single-Center Experience. Transplant. Proc. 2014;46:3459–3462. doi: 10.1016/j.transproceed.2014.08.051. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
