

Comparison of Complications in Early and Late Cranioplasty Following Decompressive Craniectomy Due to Traumatic Brain Injury: Systematic Review and Meta-Analysis
- PMID: 40565921
- PMCID: PMC12194293
- DOI: 10.3390/jcm14124176
Comparison of Complications in Early and Late Cranioplasty Following Decompressive Craniectomy Due to Traumatic Brain Injury: Systematic Review and Meta-Analysis
Abstract
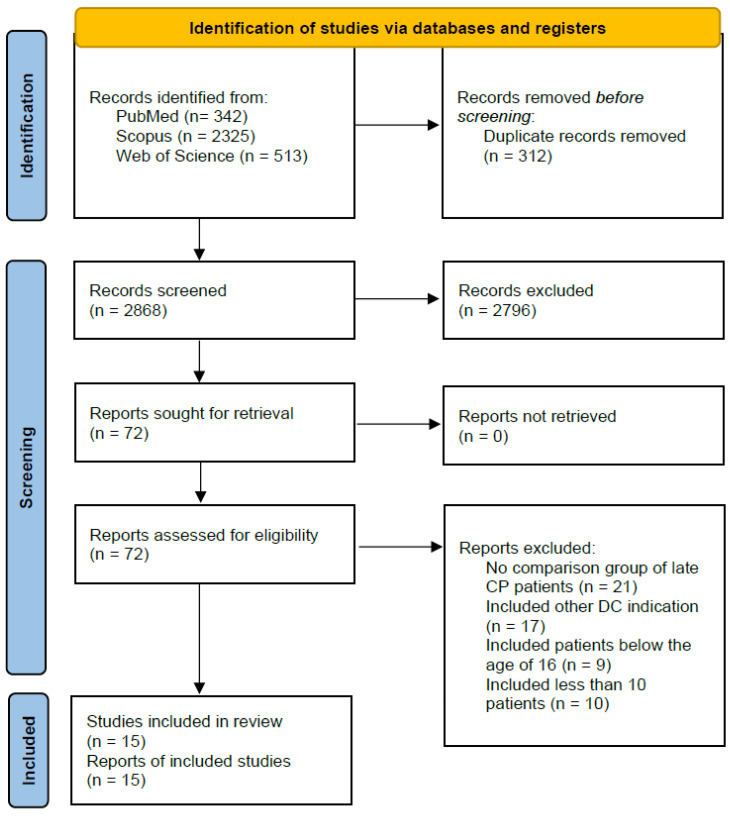
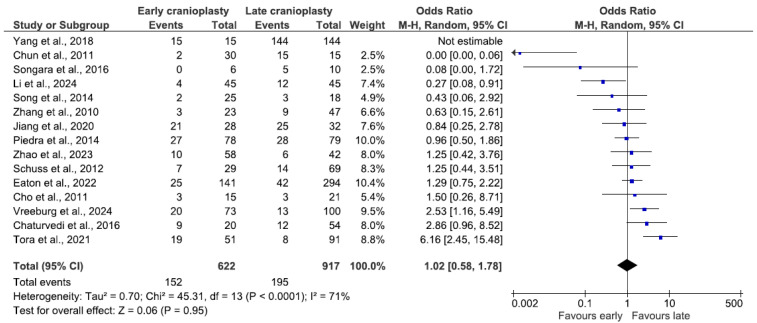
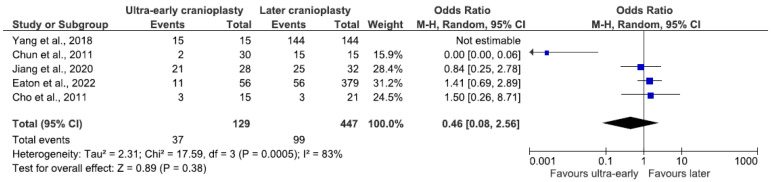
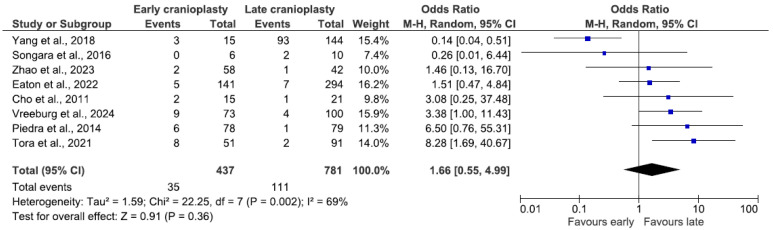
Objectives: This study investigates the relationship between the time elapsed from decompressive craniectomy to cranioplasty and surgical complications in patients after traumatic brain injury. Methods: PubMed, Scopus, and Web of Science were systematically searched for references using the PRISMA guidelines. The data were subjected to the first phase of screening, which required the studies to be published between 1990 and 2024, be written in English, and include patients who underwent cranioplasty following decompressive craniectomy due to traumatic brain injury. The second phase of screening assessed whether the studies included at least 10 patients and compared their outcomes based on the time between decompressive craniectomy and cranioplasty. A subgroup analysis was performed for ultra-early cranioplasty patients. Results: This meta-analysis included fifteen studies involving patients who underwent early (n = 666) and late cranioplasty (n = 1214) after decompressive craniectomy. All studies had a retrospective observational design. There was no statistically significant difference in the odds of complications between the groups, although late cranioplasty had slightly elevated odds of developing hydrocephalus (OR 1.66, 95% CI 0.55-4.99, p = 0.36). Interesting results stemmed from a subgroup analysis of the ultra-early cohort; they included favoring the ultra-early group in the odds of overall complications (OR 0.46, 95% CI 0.08-2.56, p = 0.38) and hygroma (OR 0.45, 95% CI 0.15-1.37, p = 0.16). Later cranioplasty had better outcomes in the category of seizure (OR 1.56, 95% CI 0.75-3.28, p = 0.24). Conclusions: Cranioplasty within 90 days, considered early, had no statistically significant differences in complication rates compared to late cranioplasty.
Keywords: complications; cranioplasty; decompressive craniectomy; traumatic brain injury.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Complications following cranioplasty and relationship to timing: A systematic review and meta-analysis.J Clin Neurosci. 2016 Nov;33:39-51. doi: 10.1016/j.jocn.2016.04.017. Epub 2016 Aug 4. J Clin Neurosci. 2016. PMID: 27499122
-
Timing Matters: A Comprehensive Meta-Analysis on the Optimal Period for Cranioplasty After Severe Traumatic Brain Injury.Oper Neurosurg. 2024 Nov 13;29(1):1-18. doi: 10.1227/ons.0000000000001404. Oper Neurosurg. 2024. PMID: 40522326
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
A systematic review and meta-analysis of factors involved in bone flap resorption after decompressive craniectomy.Neurosurg Rev. 2022 Jun;45(3):1915-1922. doi: 10.1007/s10143-022-01737-z. Epub 2022 Jan 21. Neurosurg Rev. 2022. PMID: 35061139
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
References
-
- James S.L., Theadom A., Ellenbogen R.G., Bannick M.S., Montjoy-Venning W., Lucchesi L.R., Abbasi N., Abdulkader R., Abraha H.N., Adsuar J.C., et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:56–87. doi: 10.1016/S1474-4422(18)30415-0. - DOI - PMC - PubMed
-
- Zheng F., Xu H., von Spreckelsen N., Stavrinou P., Timmer M., Goldbrunner R., Cao F., Ran Q., Li G., Fan R., et al. Early or late cranioplasty following decompressive craniotomy for traumatic brain injury: A systematic review and meta-analysis. J. Int. Med. Res. 2018;46:2503–2512. doi: 10.1177/0300060518755148. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
