

Hypertrophic Cardiomyopathy and Phenocopies: New Therapies for Old Diseases-Current Evidence and Future Perspectives
- PMID: 40565972
- PMCID: PMC12193899
- DOI: 10.3390/jcm14124228
Hypertrophic Cardiomyopathy and Phenocopies: New Therapies for Old Diseases-Current Evidence and Future Perspectives
Abstract
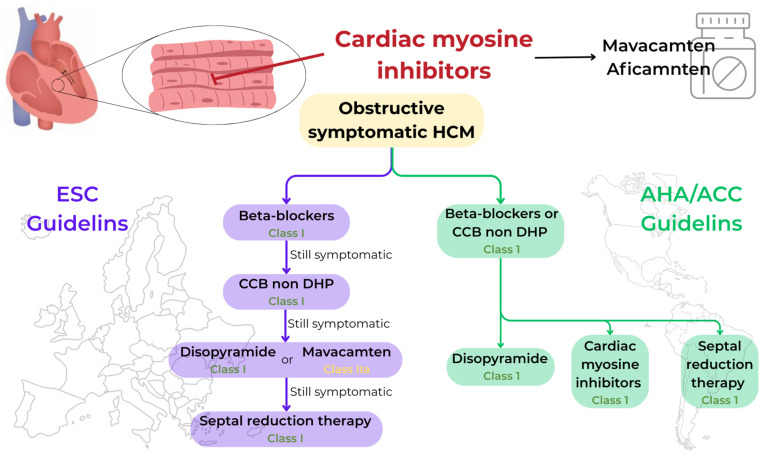
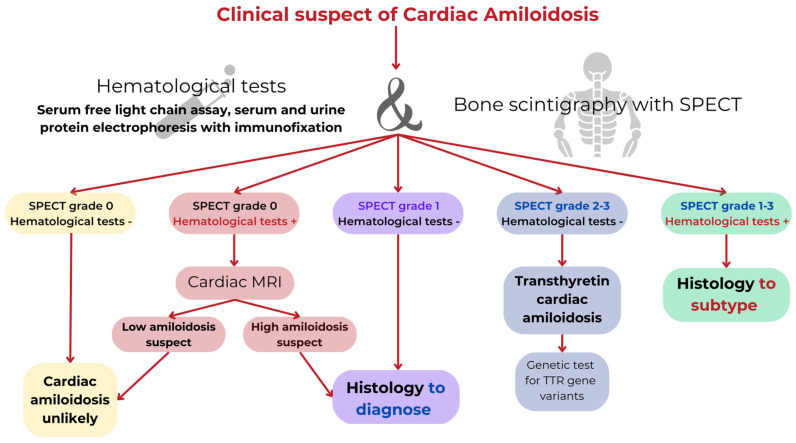
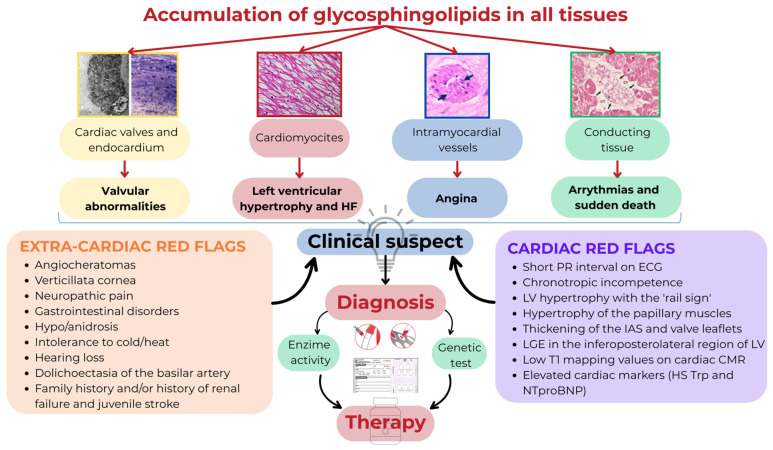
The hypertrophic cardiomyopathy (HCM) clinical phenotype includes sarcomeric HCM, which is the most common form of inherited cardiomyopathy with a population prevalence of 1:500, and phenocopies such as cardiac amyloidosis and Anderson-Fabry disease, which are considered rare diseases. Identification of cardiac and non-cardiac red flags in the context of multi-organ syndrome, multimodality imaging, including echocardiography, cardiac magnetic resonance, and genetic testing, has a central role in the diagnostic pathway. Identifying the specific disease underlying the hypertrophic phenotype is very important since many disease-modifying therapies are currently available, and phase 3 trials for new treatments have been completed or are ongoing. In particular, many chemotherapy agents (alkylating agents, proteasome inhibitors, immunomodulatory drugs, and monoclonal antibodies targeting clonal cells) allowing one to treat AL amyloidosis, transthyretin stabilizers (tafamidis and acoramidis), and gene silencers (patisiran and vutrisiran) are available in transthyretin cardiac amyloidosis, and enzyme replacement therapies (agalsidase-alpha, agalsidase-beta, and pegunigalsidase-alpha) or oral chaperone therapy (migalastat) can be used in Anderson-Fabry disease. In addition, the introduction of cardiac myosin inhibitors (mavacamten and aficamten) has deeply modified the treatment of hypertrophic obstructive cardiomyopathy. The aim of this review is to describe the new disease-modifying treatments available in HCM and phenocopies in light of current scientific evidence.
Keywords: cardiac magnetic resonance; cardiomyopathy; disease-modifying therapy; genetic test.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Comprehensive Review: Mavacamten and Aficamten in Hypertrophic Cardiomyopathy.Biomedicines. 2025 Jul 1;13(7):1619. doi: 10.3390/biomedicines13071619. Biomedicines. 2025. PMID: 40722692 Free PMC article. Review.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Laser therapy for treating hypertrophic and keloid scars.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD011642. doi: 10.1002/14651858.CD011642.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161591 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
Aficamten vs Metoprolol for Obstructive Hypertrophic Cardiomyopathy: MAPLE-HCM Rationale, Study Design, and Baseline Characteristics.JACC Heart Fail. 2025 Feb;13(2):346-357. doi: 10.1016/j.jchf.2024.11.011. JACC Heart Fail. 2025. PMID: 39909646
References
-
- Elliott P.M., Anastasakis A., Borger M.A., Borggrefe M., Cecchi F., Charron P., Hagege A.A., Lafont A., Limongelli G., Mahrholdt H., et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) Eur. Heart J. 2014;35:2733–2779. doi: 10.1093/eurheartj/ehu284. - DOI - PubMed
-
- Maron B.J., Rowin E.J., Maron M.S. Global burden of hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2018;6:376–378. doi: 10.1016/j.jchf.2018.03.004. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
