

Understanding the Perioperative Perception of Pain in Patients with Crohn's Disease: Epidural Versus Non-Epidural Analgesia
- PMID: 40566130
- PMCID: PMC12193785
- DOI: 10.3390/jcm14124383
Understanding the Perioperative Perception of Pain in Patients with Crohn's Disease: Epidural Versus Non-Epidural Analgesia
Abstract
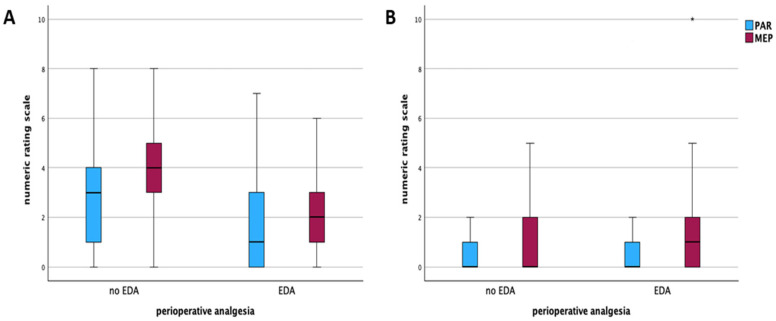
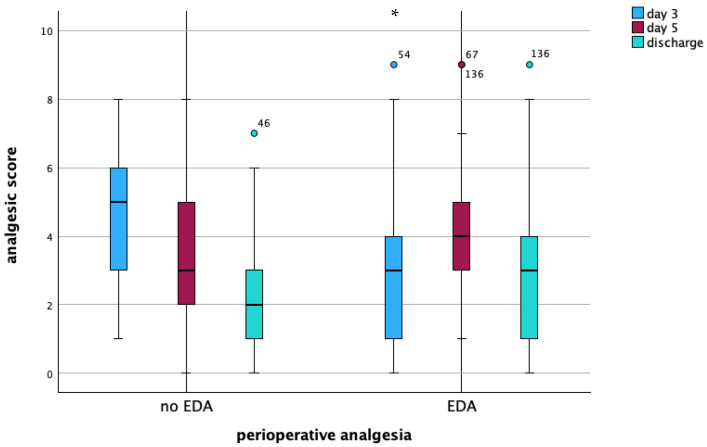
Background: Patients with Crohn's disease (CD) suffer from a relevant burden of abdominal pain and psychological distress that can aggravate postoperatively. While systematic strategies for postoperative pain management are lacking, the potential benefit of perioperative epidural analgesia (EDA) in CD patients is unclear. Methods: All patients receiving an ileocecal resection due to CD at a tertiary hospital were included. The impact of epidural versus non-epidural analgesia on postoperative pain perception was evaluated by analyzing the numeric rating scale (NRS), analgesic consumption, and clinical outcomes. Results: In this monocentric study, 172 patients receiving ileocecal resection due to CD were included, with 122 receiving EDA. The epidural pain catheters were kept for an average of 4.4 days (±1.3) before being removed. EDA resulted in significantly decreased pain as well as a decreased amount of analgesic consumption (adjuvant analgesics: 16.4% vs. 32%, p = 0.021; strong opioids: 30.3% vs. 72.0%, p < 0.001) at the early postoperative course (1 vs. 3 at rest and 2 vs. 4 movement-evoked, p < 0.001). No difference in pain perception was detected on day 5 between EDA and non-EDA patients. Patients with EDA had a significantly longer length of hospital stay (7.5 versus 6 days, p = 0.002) and an increased intake of weak opioids at discharge (p = 0.024). Conclusions: While EDA in CD patients resulted in significantly decreased pain and decreased amounts of analgesic adjuvants and strong opioids at the early postoperative course, intravenous and oral analgesia provide sufficient postoperative pain control after surgery and earlier patient autonomy.
Keywords: Crohn’s disease; colorectal surgery; pain management; perioperative medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults.Cochrane Database Syst Rev. 2018 Jun 4;6(6):CD009642. doi: 10.1002/14651858.CD009642.pub3. Cochrane Database Syst Rev. 2018. PMID: 29864216 Free PMC article.
-
Pain management for women in labour: an overview of systematic reviews.Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD009234. doi: 10.1002/14651858.CD009234.pub2. Cochrane Database Syst Rev. 2012. PMID: 22419342 Free PMC article.
-
Patient-controlled analgesia with remifentanil versus alternative parenteral methods for pain management in labour.Cochrane Database Syst Rev. 2017 Apr 13;4(4):CD011989. doi: 10.1002/14651858.CD011989.pub2. Cochrane Database Syst Rev. 2017. PMID: 28407220 Free PMC article.
-
Epidural versus non-epidural or no analgesia for pain management in labour.Cochrane Database Syst Rev. 2018 May 21;5(5):CD000331. doi: 10.1002/14651858.CD000331.pub4. Cochrane Database Syst Rev. 2018. PMID: 29781504 Free PMC article.
-
Interventions for the management of abdominal pain in Crohn's disease and inflammatory bowel disease.Cochrane Database Syst Rev. 2021 Nov 29;11(11):CD013531. doi: 10.1002/14651858.CD013531.pub2. Cochrane Database Syst Rev. 2021. PMID: 34844288 Free PMC article.
References
-
- Ng S.C., Shi H.Y., Hamidi N., Underwood F.E., Tang W., Benchimol E.I., Panaccione R., Ghosh S., Wu J.C.Y., Chan F.K.L., et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet. 2017;390:2769–2778. doi: 10.1016/S0140-6736(17)32448-0. - DOI - PubMed
LinkOut - more resources
Full Text Sources
